Late-Onset Postpneumonectomy Empyema Presenting as Right-Sided Heart Failure: Extrinsic Right Atrial Compression
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Inje University College of Medicine, Ilsan Paik Hospital, Goyang, Korea. jnamgung@paik.ac.kr
- 2Department of Thoracic Surgery, Inje University College of Medicine, Ilsan Paik Hospital, Goyang, Korea.
- 3Department of Radiology, Inje University College of Medicine, Ilsan Paik Hospital, Goyang, Korea.
- KMID: 2225021
- DOI: http://doi.org/10.4070/kcj.2012.42.4.274
Abstract
- Although it is rare, the right atrium can be encroached on by abnormal mediastinal structures, including aortic aneurysms, carcinomas, hepatic cysts and diaphragmatic paralysis. Extrinsic compression of the right atrium causes significant hemodynamic compromise and can lead to fatal outcomes. We describe the case of a 66-year old man with a past history of pulmonary tuberculosis that had undergone right pneumonectomy 40 years previously. He then presented with signs and symptoms of right-sided heart failure. These new signs and symptoms were recognized to be secondary to extrinsic compression of the right atrium, which was due to late-onset postpneumonectomy empyema, and the signs and symptoms were successfully relieved by performing open drainage of the empyema.
MeSH Terms
Figure
-
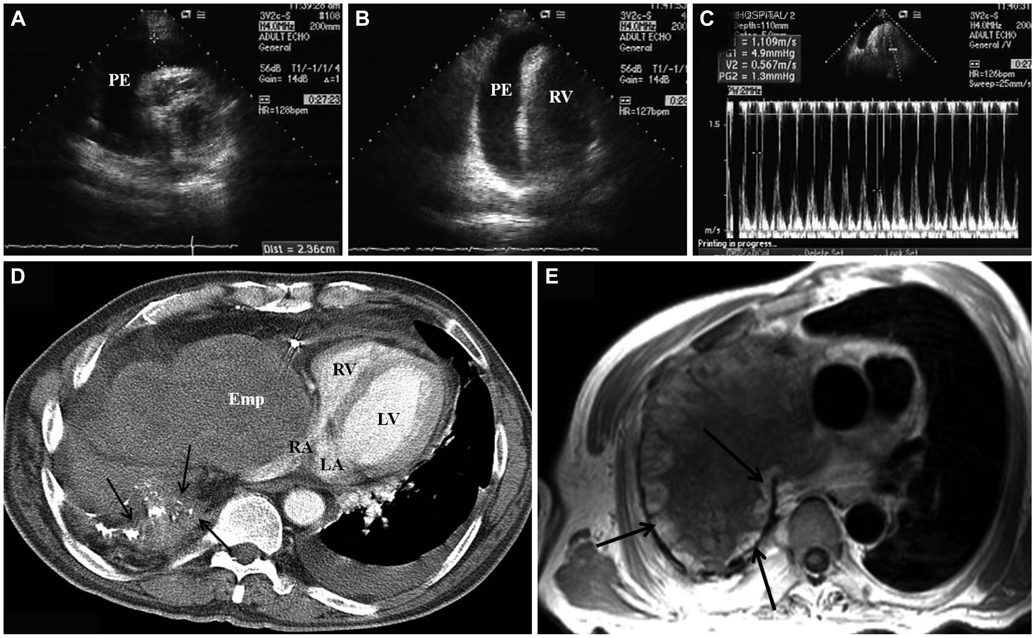
Fig. 1 A and B: a short-axis and an apical 4-chamber transthoracic echocardiography view demonstrated a pericardial effusion of over 2 cm around the free wall of the right ventricle. C: respiratory variations of transmitral Doppler inflow: a decrease of peak flow velocity with >25% (from 1.1 to 0.5 m/s) during inspiration. D: post contrast CT at the level of the left ventricle. The large mass with a mean CT number of 40 is empyema. Note the thick pleura with calcifications (arrows), and this represents a fibrothorax from the tuberculosis. The right atrium is markedly compressed by the empyema. A small to moderate amount of left pleural effusion is noted (the mean CT number is 25). E: axial image of chest MRI. A large mass in the right thorax compresses the right heart and vena cava. The mass has a lobular fibrous capsule of high signal intensity and a central low signal intensity. The thick fibrous capsule shows various degrees of enhancement (arrows). FA of 180 degrees, a TR of 976 milliseconds and a TE of 12 milliseconds. PE: pericardial effusion, Emp: empyema, RA: right atrium, RV: right ventricle, LA: left atrium, LV: left ventricle.
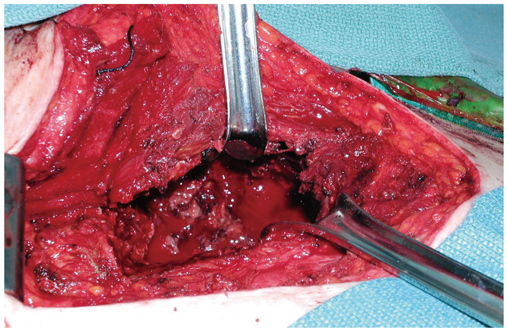
Fig. 2 Partial resection of right 4th and 5th rib was peformed. The operative field showed a large amount of empyema debris filled in the right pleural cavity.
Reference
-
1. D'Cruz IA, Feghali N, Gross CM. Echocardiographic manifestations of mediastinal masses compressing or encroaching on the heart. Echocardiography. 1994. 11:523–533.2. Fowler NO, Gabel M, Buncher CR. Cardiac tamponade: a comparison of right versus left heart compression. J Am Coll Cardiol. 1988. 12:187–193.3. Kerr WF. Late-onset post-pneumonectomy empyema. Thorax. 1977. 32:149–154.4. Model D. Occult empyema presenting ten years after pneumonectomy. Lancet. 1983. 1:192–193.5. Rogiers P, Van Mieghem W, Engelaar D, Demedts M. Late-onset post-pneumonectomy empyema manifesting as tracheal stenosis with respiratory failure. Respir Med. 1991. 85:333–335.6. Stafford EG, Clagett OT. Postpneumonectomy emphema: neomycin instillation and definitive closure. J Thorac Cardiovasc Surg. 1972. 63:771–775.7. Berge MV, Snoek WJ, Nijboer EW, Julius AJ, Aalbers R. A man with upper respiratory tract infections, general weakness and fever. Eur Respir J. 1999. 14:469–470.8. Moon JY, Jeong HC, Cho JY, et al. Anomalous origin of a right coronary artery with extrinsic compression between the great vessels: the intravascular ultrasound images. Korean Circ J. 2008. 38:390–392.9. Goldstraw P. Treatment of postpneumonectomy empyema: the case for fenestration. Thorax. 1979. 34:740–745.10. Wain JC. Management of late postpneumonectomy empyema and bronchopleural fistula. Chest Surg Clin N Am. 1996. 6:529–541.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical treatment of postpneumonectomy empyema with bronchopleural fistula: 2 cases using pedicled omental flap & muscle transposition
- Acute Postpneumonectomy Empyema with Bronchopleural Fistula Treated with Vacuum-assisted Closure Device
- Application of Vacuum-Assisted Closure Device in Management of Postpneumonectomy Empyema
- Pathophysiology and Diagnosis in Atrial Fibrillation
- Anesthetic Management of a Patient with Postpneumonectomy Syndrome for Corrective Surgery: A case report
