Korean Circ J.
2013 May;43(5):340-342. 10.4070/kcj.2013.43.5.340.
Acquired Long QT Syndrome Manifesting with Torsades de Pointes in a Patient with Panhypopituitarism due to Radiotherapy
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kangdong Sacred Heart Hospital, Hallym University Medical Center, Seoul, Korea. drhyangii@hallym.or.kr
- KMID: 2224931
- DOI: http://doi.org/10.4070/kcj.2013.43.5.340
Abstract
- We describe a 64-year-old male patient with panhypopituitarism who experienced polymorphic ventricular tachycardia (VT) associated with long QT intervals. The panhypopituitarism developed as a sequelae of radiation therapy administered 20 years prior to his current presentation and was recently aggravated by urinary tract infection with sepsis. In this case, polymorphic VT was resistant to conventional therapy (including magnesium infusion), and QT prolongation and T wave inversion were normalized after the administration of steroid and thyroid hormones. Thyroid hormone is generally known to be associated with torsades de pointes (TdP), but steroid or other hormones may also provoke TdP. Hormonal disorders should be considered as a cause of polymorphic VT with long QT intervals. Some arrhythmias can be life-threatening, and they can be prevented with supplementation of the insufficient hormone.
MeSH Terms
Figure
-
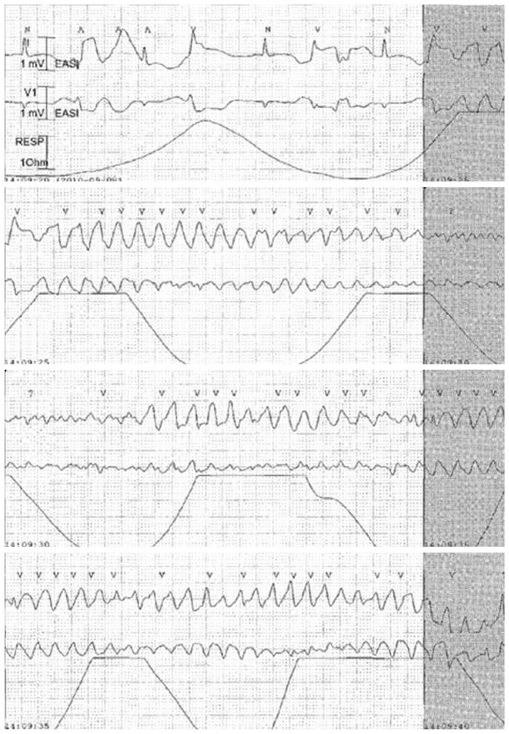
Fig. 1 Electrocardiography conducted at the hospital on day 4 showed a section of TdP rhythm during a 20-second period.
Reference
-
1. Roden DM. A practical approach to torsade de pointes. Clin Cardiol. 1997; 20:285–290.2. Molokhia M, Pathak A, Lapeyre-Mestre M, et al. Case ascertainment and estimated incidence of drug-induced long-QT syndrome: study in Southwest France. Br J Clin Pharmacol. 2008; 66:386–395.3. Sanaei-Zadeh H, Shahmohammadi F, Zamani N, Mostafazadeh B. Can death unrelated to secondary causes be predicted in intubated comatose tricyclic antidepressant-poisoned patients? Clin Toxicol (Phila). 2011; 49:379–384.4. Hume-Smith HV, Sanatani S, Lim J, Chau A, Whyte SD. The effect of propofol concentration on dispersion of myocardial repolarization in children. Anesth Analg. 2008; 107:806–810.5. Shojaie M, Eshraghian A. Primary hypothyroidism presenting with Torsades de pointes type tachycardia: a case report. Cases J. 2008; 1:298.6. Schenck JB, Rizvi AA, Lin T. Severe primary hypothyroidism manifesting with torsades de pointes. Am J Med Sci. 2006; 331:154–156.7. Nishizawa S, Nakamura T, Hamaoka T, Matsumuro A, Sawada T, Matsubara H. Lethal arrhythmia and corticosteroid insufficiency. Am J Emerg Med. 2009; 27:1167.e1–1167.e3.8. Kim NH, Cho JG, Ahn YK, et al. A case of torsade de pointes associated with hypopituitarism due to hemorrhagic fever with renal syndrome. J Korean Med Sci. 2001; 16:355–359.9. Izumi C, Inoko M, Kitaguchi S, et al. Polymorphic ventricular tachycardia in a patient with adrenal insufficiency and hypothyroidism. Jpn Circ J. 1998; 62:543–545.10. Hartog M, Joplin GF. Effects of cortisol deficiency on the electrocardiogram. Br Med J. 1968; 2:275–277.11. Takimoto K, Levitan ES. Glucocorticoid induction of Kv1.5 K+ channel gene expression in ventricle of rat heart. Circ Res. 1994; 75:1006–1013.12. Iga K, Hori K, Gen H. Deep negative T waves associated with reversible left ventricular dysfunction in acute adrenal crisis. Heart Vessels. 1992; 7:107–111.13. Sauer AJ, Moss AJ, McNitt S, et al. Long QT syndrome in adults. J Am Coll Cardiol. 2007; 49:329–337.14. Odening KE, Choi BR, Koren G. Sex hormones and cardiac arrest in long QT syndrome: does progesterone represent a potential new antiarrhythmic therapy? Heart Rhythm. 2012; 9:1150–1152.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Cardiac Arrest Related to Torsades de Pointes in a Patient Recovering from Diabetic Ketoacidosis
- Initiation of Torsades de pointes by head-up tilt test in congenital long QT syndrome patient
- A Case of Torsades de Pointes Induced by Cisapride
- Torsades de pointes observed in the early postoperative period in a patient with long QT syndrome
- Clinical Experience for a Patient with Long QT Syndrome
