Korean Circ J.
2013 Aug;43(8):527-533. 10.4070/kcj.2013.43.8.527.
Predictors of Recovery of Left Ventricular Systolic Dysfunction after Acute Myocardial Infarction: From the Korean Acute Myocardial Infarction Registry and Korean Myocardial Infarction Registry
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Gil Hospital, Gachon University, Incheon, Korea. encore@gilhospital.com
- 2Division of Cardiology, Department of Internal Medicine, Chonnam National University, Gwangju, Korea.
- KMID: 2224842
- DOI: http://doi.org/10.4070/kcj.2013.43.8.527
Abstract
- BACKGROUND AND OBJECTIVES
We investigated the predictors of the recovery of depressed left ventricular ejection fraction (LVEF) in patients with moderate or severe left ventricular (LV) systolic dysfunction after acute myocardial infarction (MI).
SUBJECTS AND METHODS
We analyzed 1307 patients, who had moderately or severely depressed LVEF (<45%) on echocardiography soon after acute MI and who underwent a follow-up echocardiography, among 27369 patients from the Korea Working Group on the Myocardial Infarction Registry. Patients were categorized into two groups according to recovery of LVEF: group I with consistently depressed LVEF (<45%) at the follow-up echocardiography and group II with a recovery of LVEF (> or =45%).
RESULTS
Recovery of LV systolic dysfunction was observed in 51% of the subjects (group II, n=663; DeltaLVEF, 16.2+/-9.3%), whereas there was no recovery in the remaining subjects (group I, n=644; DeltaLVEF, 0.6+/-7.1%). In the multivariate analysis, independent predictors of recovery of depressed LVEF were as follows {odds ratio (OR) [95% confidence interval (CI)]}: moderate systolic dysfunction {LVEF > or =30% and <45%; 1.73 (1.12-2.67)}, Killip class I-II {1.52 (1.06-2.18)}, no need for diuretics {1.59 (1.19-2.12)}, non-ST-segment elevation MI {1.55 (1.12-2.16)}, lower peak troponin I level {<24 ng/mL, median value; 1.55 (1.16-2.07)}, single-vessel disease {1.53 (1.13-2.06)}, and non-left anterior descending (LAD) culprit lesion {1.50 (1.09-2.06)}. In addition, the use of statin was independently associated with a recovery of LV systolic dysfunction {OR (95% CI), 1.46 (1.07-2.00)}.
CONCLUSION
Future contractile recovery of LV systolic dysfunction following acute MI was significantly related with less severe heart failure at the time of presentation, a smaller extent of myonecrosis, or non-LAD culprit lesions rather than LAD lesions.
MeSH Terms
Figure
-
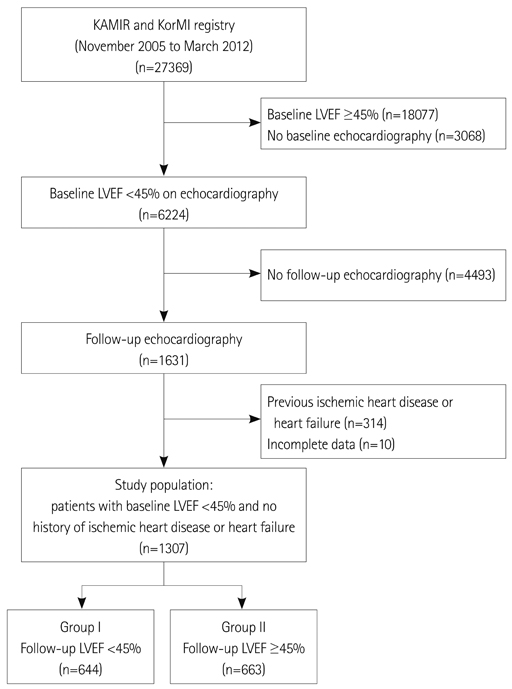
Fig. 1 The flow chart of the study. KAMIR: Korean Acute Myocardial Infarction Registry, KorMI: Korean Myocardial Infarction, LVEF: left ventricular ejection fraction.
Cited by 1 articles
-
Therapeutic Hypothermia for Cardioprotection in Acute Myocardial Infarction
In Sook Kang, Ikeno Fumiaki, Wook Bum Pyun
Yonsei Med J. 2016;57(2):291-297. doi: 10.3349/ymj.2016.57.2.291.
Reference
-
1. Risk stratification and survival after myocardial infarction. N Engl J Med. 1983; 309:331–336.2. White HD, Norris RM, Brown MA, Brandt PW, Whitlock RM, Wild CJ. Left ventricular end-systolic volume as the major determinant of survival after recovery from myocardial infarction. Circulation. 1987; 76:44–51.3. St John Sutton M, Pfeffer MA, Plappert T, et al. Quantitative two-dimensional echocardiographic measurements are major predictors of adverse cardiovascular events after acute myocardial infarction. The protective effects of captopril. Circulation. 1994; 89:68–75.4. Gaudron P, Eilles C, Kugler I, Ertl G. Progressive left ventricular dysfunction and remodeling after myocardial infarction. Potential mechanisms and early predictors. Circulation. 1993; 87:755–763.5. Bolognese L, Cerisano G, Buonamici P, et al. Influence of infarct-zone viability on left ventricular remodeling after acute myocardial infarction. Circulation. 1997; 96:3353–3359.6. Christian TF, Behrenbeck T, Pellikka PA, Huber KC, Chesebro JH, Gibbons RJ. Mismatch of left ventricular function and infarct size demonstrated by technetium-99m isonitrile imaging after reperfusion therapy for acute myocardial infarction: identification of myocardial stunning and hyperkinesia. J Am Coll Cardiol. 1990; 16:1632–1638.7. Wijns W, Vatner SF, Camici PG. Hibernating myocardium. N Engl J Med. 1998; 339:173–181.8. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005; 18:1440–1463.9. Ottervanger JP, van't Hof AW, Reiffers S, et al. Long-term recovery of left ventricular function after primary angioplasty for acute myocardial infarction. Eur Heart J. 2001; 22:785–790.10. Leclercq F, Messner-Pellenc P, Moragues C, et al. Myocardial viability assessed by dobutamine echocardiography in acute myocardial infarction after successful primary coronary angioplasty. Am J Cardiol. 1997; 80:6–10.11. Abdel-Salam Z, Nammas W. Predictors of myocardial contractile recovery after coronary revascularization in patients with prior myocardial infarction. Cardiovasc Revasc Med. 2010; 11:2–7.12. Gibbons RJ, Valeti US, Araoz PA, Jaffe AS. The quantification of infarct size. J Am Coll Cardiol. 2004; 44:1533–1542.13. Solomon SD, Glynn RJ, Greaves S, et al. Recovery of ventricular function after myocardial infarction in the reperfusion era: the healing and early afterload reducing therapy study. Ann Intern Med. 2001; 134:451–458.14. Bauters C, Fertin M, Delhaye C, et al. Late recovery in left ventricular systolic function after discharge of patients with a first anterior myocardial infarction. Arch Cardiovasc Dis. 2010; 103:538–545.15. Steen H, Futterer S, Merten C, Jünger C, Katus HA, Giannitsis E. Relative role of NT-pro BNP and cardiac troponin T at 96 hours for estimation of infarct size and left ventricular function after acute myocardial infarction. J Cardiovasc Magn Reson. 2007; 9:749–758.16. Eitzman D, al-Aouar Z, Kanter HL, et al. Clinical outcome of patients with advanced coronary artery disease after viability studies with positron emission tomography. J Am Coll Cardiol. 1992; 20:559–565.17. Auerbach MA, Schöder H, Hoh C, et al. Prevalence of myocardial viability as detected by positron emission tomography in patients with ischemic cardiomyopathy. Circulation. 1999; 99:2921–2926.18. Stenestrand U, Wallentin L. Swedish Register of Cardiac Intensive Care (RIKS-HIA). Early statin treatment following acute myocardial infarction and 1-year survival. JAMA. 2001; 285:430–436.19. Horwich TB, MacLellan WR, Fonarow GC. Statin therapy is associated with improved survival in ischemic and non-ischemic heart failure. J Am Coll Cardiol. 2004; 43:642–648.20. Kjekshus J, Pedersen TR, Olsson AG, Faergeman O, Pyörälä K. The effects of simvastatin on the incidence of heart failure in patients with coronary heart disease. J Card Fail. 1997; 3:249–254.21. Aronow WS, Ahn C. Frequency of congestive heart failure in older persons with prior myocardial infarction and serum low-density lipoprotein cholesterol > or = 125 mg/dl treated with statins versus no lipid-lowering drug. Am J Cardiol. 2002; 90:147–149.22. Sola S, Mir MQ, Lerakis S, Tandon N, Khan BV. Atorvastatin improves left ventricular systolic function and serum markers of inflammation in nonischemic heart failure. J Am Coll Cardiol. 2006; 47:332–337.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Can time delay be shortened in the treatment of acute myocardial infarction?: Experience from Korea acute myocardial infarction registry
- Invasive Treatment of Acute Myocardial Infarction: What is the Optimal Therapy for Acute Myocardial Infarction?
- Incidence of Left Ventricular Thrombus after Acute Myocardial Infarction
- A Case of the Thrombi in Left Atrial Appendage Confirmed by Transesophageal Echocardiography(TEE) in A Patient with Acute Myocardial Infarction Accompanied by Cerebral Infarction
- Two-Dimensional Echocardiographic Predictors of Ventricular Enlargement after Acute Myocardial Infarction
