Acute ST Elevated Myocardial Injury due to Coronary Thrombosis during Thoracic Endovascular Aortic Repair in Patient with Protein S Deficiency
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Sejong General Hospital, Bucheon, Korea. whshim@yuhs.ac
- KMID: 2223860
- DOI: http://doi.org/10.4070/kcj.2014.44.6.429
Abstract
- A 71-year-old woman who had suffered from pulmonary thromboembolism with deep vein thrombosis for 12 years presented the hospital with a huge thoracic aortic aneurysm. During thoracic endovascular therapy, she had a sudden coronary artery occlusion without having organized stenosis or plaque rupture even under the dual antiplatelet treatment and heparinization. She turned out to be having a protein S deficiency. A procedure related thrombotic adverse event in patient with protein S deficiency is very rare, so we report a case with literature review.
Keyword
MeSH Terms
Figure
-
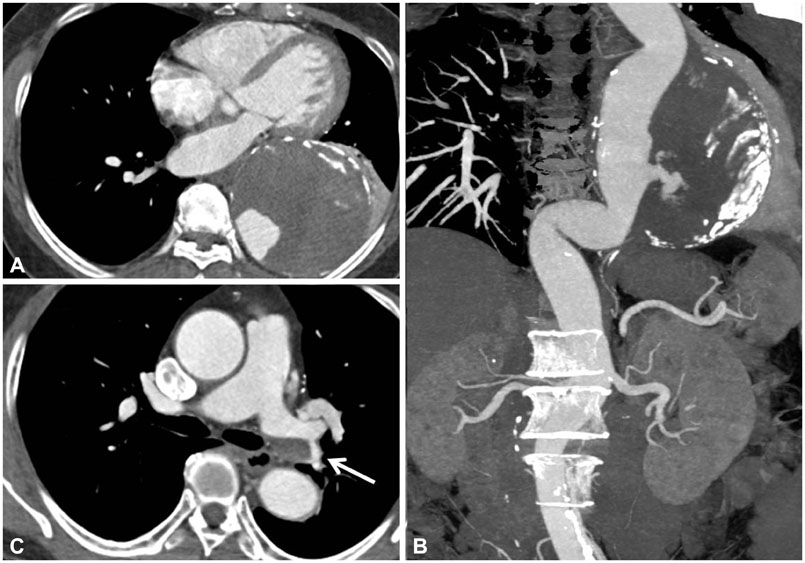
Fig. 1 Pre-procedural aorta CT of presented patient. A: axial CT image shows the huge aneurysm (11 cm of diameter) containing the thrombus. B: reconstructed CT image shows the huge aneurysm containing the mural thrombus and the contrast leakage is seen inside the aneurysm as well. C: axial CT image shows the organized thrombi at the left main pulmonary artery.
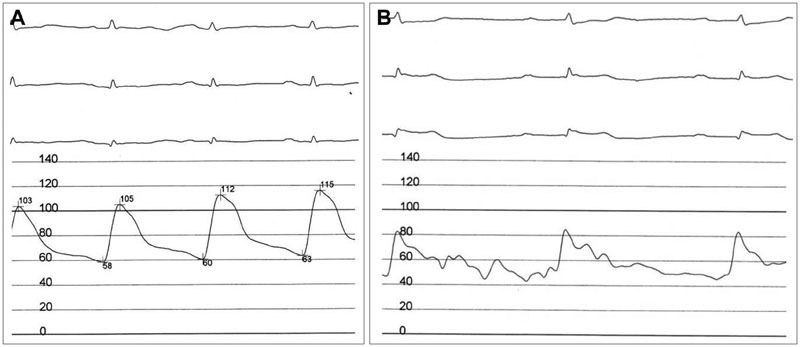
Fig. 2 Baseline and the event polygraphic records show the 3 limb leads ECG and the pulse pressure at the right common femoral artery sheath. A: baseline ECG shows 70 beats per minute of heart rate without significant ST height difference and blood pressure is approximately 110/60 mm Hg. B: an ECG at the time of chest pain indicates newly developed ST elevation at avF limb lead compared to the baseline ECG with 45 beats per minute of heart rate and the blood pressure is approximately 80/50 mm Hg. ECG: electrocardiography.
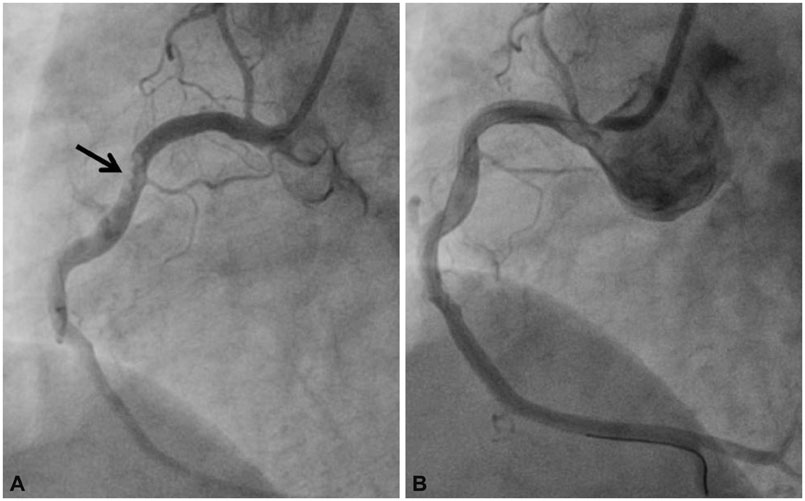
Fig. 3 Right coronary artery angiography before and after the thrombus aspiration. A: right coronary angiography shows the mobile multiple thrombi inside of the vessels and the TIMI grade 1 of blood flow. B: right coronary angiography after the thrombus aspiration shows no organic stenosis or remnant thrombi inside the vessel and the TIMI grade 4 of blood flow is restored. TIMI: Thrombolysis in Myocardial Infarction.

Fig. 4 A pig-tail aortogram and CT angiography after stent-graft insertion. A: a aortogram shows the good position of stent-graft without any kind of leakage. B: a CT angiography taken before discharge shows complete coverage of aneurysm.
Reference
-
1. Walsh SR, Tang TY, Sadat U, et al. Endovascular stenting versus open surgery for thoracic aortic disease: systematic review and meta-analysis of perioperative results. J Vasc Surg. 2008; 47:1094–1098.2. Desai ND, Burtch K, Moser W, et al. Long-term comparison of thoracic endovascular aortic repair (TEVAR) to open surgery for the treatment of thoracic aortic aneurysms. J Thorac Cardiovasc Surg. 2012; 144:604–609. discussion 609-11.3. Mateo J, Oliver A, Borrell M, Sala N, Fontcuberta J. Laboratory evaluation and clinical characteristics of 2,132 consecutive unselected patients with venous thromboembolism--results of the Spanish Multicentric Study on Thrombophilia (EMET-Study). Thromb Haemost. 1997; 77:444–451.4. Allaart CF, Aronson DC, Ruys T, et al. Hereditary protein S deficiency in young adults with arterial occlusive disease. Thromb Haemost. 1990; 64:206–210.5. Douay X, Lucas C, Caron C, Goudemand J, Leys D. Antithrombin, protein C and protein S levels in 127 consecutive young adults with ischemic stroke. Acta Neurol Scand. 1998; 98:124–127.6. Lee WA, Brown MP, Nelson PR, Huber TS. Total percutaneous access for endovascular aortic aneurysm repair ("Preclose" technique). J Vasc Surg. 2007; 45:1095–1101.7. Sukhija R, Aronow WS, Yalamanchili K, Sinha N, Babu S. Prevalence of coronary artery disease, lower extremity peripheral arterial disease, and cerebrovascular disease in 110 men with an abdominal aortic aneurysm. Am J Cardiol. 2004; 94:1358–1359.8. Bub GL, Greenberg RK, Mastracci TM, et al. Perioperative cardiac events in endovascular repair of complex aortic aneurysms and association with preoperative studies. J Vasc Surg. 2011; 53:21–27.e1-2.9. Wang GJ, Fairman RM, Jackson BM, Szeto WY, Pochettino A, Woo EY. The outcome of thoracic endovascular aortic repair (TEVAR) in patients with renal insufficiency. J Vasc Surg. 2009; 49:42–46.10. Engesser L, Broekmans AW, Briët E, Brommer EJ, Bertina RM. Hereditary protein S deficiency: clinical manifestations. Ann Intern Med. 1987; 106:677–682.11. Munts AG, van Genderen PJ, Dippel DW, van Kooten F, Koudstaal PJ. Coagulation disorders in young adults with acute cerebral ischaemia. J Neurol. 1998; 245:21–25.12. Beattie S, Norton M, Doll D. Coronary thrombosis associated with inherited protein S deficiency: a case report. Heart Lung. 1997; 26:76–79.13. Carrié D, Béard T, Sié P, Boudjemaa B, Delay M, Bernadet P. [Simultaneous thrombosis of the left anterior interventricular and right coronary arteries in a 27 year-old patient with protein S deficiency]. Arch Mal Coeur Vaiss. 1993; 86:921–924.14. Manzar KJ, Padder FA, Conrad AR, Freeman I, Jonas EA. Acute myocardial infarction with normal coronary artery: a case report and review of literature. Am J Med Sci. 1997; 314:342–345.15. Schwarz HP, Fischer M, Hopmeier P, Batard MA, Griffin JH. Plasma protein S deficiency in familial thrombotic disease. Blood. 1984; 64:1297–1300.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Thrombotic Occlusion of Left Internal Jugular Vein Compressed by Bypass Graft for Thoracic Endovascular Aortic Repair Debranching Procedure
- Acute Type B Aortic Dissection in a Patient with Previous Endovascular Abdominal Aortic Aneurysm Repair
- Endovascular Repair of Thoracic Aortic Aneurysm Using a Custom-made Fenestrated Stent Graft to Preserve the Left Subclavian Artery
- Retrograde Aortic Dissection after Thoracic Endovascular Aortic Repair for Descending Aorta: 2 case reports
- Surgical Repair of Retrograde Type A Aortic Dissection after Thoracic Endovascular Aortic Repair
