Brachial Plexus Injury Caused by Indwelling Axillary Venous Pacing Leads
- Affiliations
-
- 1Department of Cardiology, Dong-A University Medical Center, Busan, Korea. thinkmed@dau.ac.kr
- 2Department of Cardiovascular Surgery, Dong-A University Medical Center, Busan, Korea.
- 3Department of Radiology, Dong-A University Medical Center, Busan, Korea.
- KMID: 2223808
- DOI: http://doi.org/10.4070/kcj.2015.45.5.428
Abstract
- A 64-year-old male patient underwent cardiac resynchronization therapy (CRT) device implantation via the axillary venous approach. Two weeks later, the patient started complaining of "electric shock-like" pain in the left axillary area. During physical examination, typical pain in the left axillary area was reproduced whenever his left shoulder was passively abducted more than 60 degrees. Fluoroscopic examination showed that the left ventricle (LV) and right atrium (RA) leads were positioned at an acute angle directing towards the left brachial plexus whenever the patient's shoulder was passively abducted. Brachial plexus irritation by the angulated CRT leads was strongly suspected. To relieve the acute angulation, we had to adjust the entry site of the LV and RA leads from the distal to the proximal axillary vein using the cut-down method. After successful lead repositioning, the neuropathic pain improved rapidly. Although transvenous pacing lead-induced nerve injury is not a frequent complication, this possibility should be kept in mind by the operators.
Keyword
MeSH Terms
Figure
-

Fig. 1 Chest computed tomography images. A, B, and C: axial images showing an RV lead (arrows) running into the left subclavian vein at the medial side of the pectoralis minor muscle (asterisks). The LV and RA leads (arrowheads) were running together along the lateral side of the pectoralis minor muscle into the left axillary vein at the outer border of the first rib (D). A three-dimensional volume-rendered image showing overall directions of each lead. The LV and RA leads were forming a curvature with an acute angle (empty arrow) before insertion into the left axillary vein. There were no specific findings of vascular complication or local infection. RV: right ventricle, LV: left ventricle, RA: right atrium.

Fig. 2 Fluoroscopic examination images. A: fluoroscopic examination in the supine position showed the LV and RA leads inserted nearly vertically (asterisk) into the lateral axillary vein. B: active or passive shoulder abduction more than 60 degrees induced an acute angulation (empty arrowhead) of the LV and RA leads directing towards the left brachial plexus (Video in the online-only Data Supplement). Severe axillary and radiating upper extremity pain recurred whenever the LV and RA leads formed an acute angulation. C: left arm venography demonstrated that the extravascular portion of the LV and RA leads formed an acute angulation. D: the operators decided to move the initial insertion site (asterisk) of the LV and RA leads to a more proximal site at a 3 cm distance (arrow). E: after adjusting the insertion site of the LV and RA leads, the initially noted vertical insertion of the leads was not observed (F) and acute angulation of the LV and RA leads did not occur during passive shoulder abduction more than 60 degrees. LV: left ventricle, RA: right atrium.
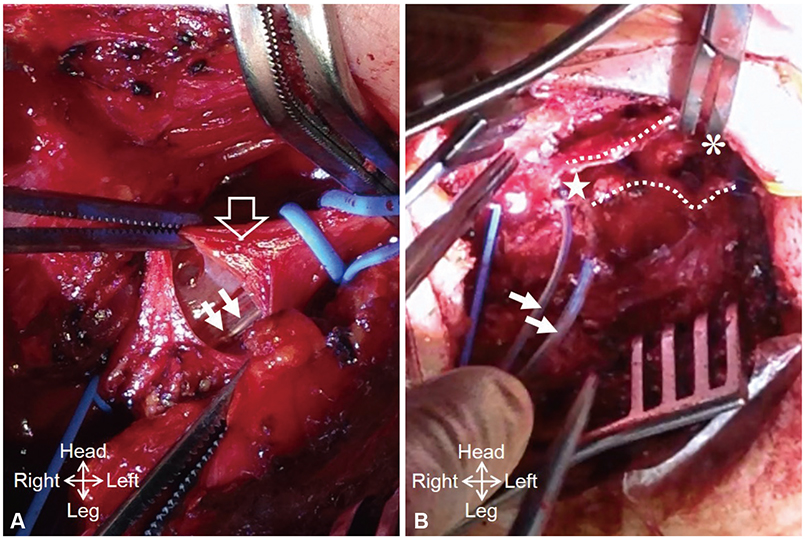
Fig. 3 Operation field findings. A: the left axillary vein (empty arrow) was exposed and incised transversely at the medial site. However, the LV and RA leads (arrows) were tightly adhered to the posterior wall of the vein, and it was impossible to manually extract them through the transverse incision line. B: the left axillary vein was incised longitudinally (dotted lines show the cutting edges) from the initial insertion site (asterisk) of the LV and RA leads to the more proximal site (star) at a 3 cm distance. After separation from the axillary venous wall, the LV and RA leads (arrows) were moved proximally and the remaining incision lines were closed. LV: left ventricle, RA: right atrium.
Reference
-
1. Kim KH, Park KM, Nam GB, et al. Comparison of the axillary venous approach and subclavian venous approach for efficacy of permanent pacemaker implantation. 8-Year follow-up results. Circ J. 2014; 78:865–871.2. Pozo E, González-Ferrer JJ, Pérez Villacastín J, Macaya C. Diaphragm paralysis due to pseudoaneurysm of internal mammary artery after pacemaker implantation. Europace. 2011; 13:592–593.3. Harris K, Maniatis G, Siddiqui F, Maniatis T. Phrenic nerve injury and diaphragmatic paralysis following pacemaker pulse generator replacement. Heart Lung. 2013; 42:65–66.4. Ramza BM, Rosenthal L, Hui R, et al. Safety and effectiveness of placement of pacemaker and defibrillator leads in the axillary vein guided by contrast venography. Am J Cardiol. 1997; 80:892–896.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Proximal Median Neuropathy Caused by Axillary Brachial Plexus Block
- Persistent Brachial Plexus Injury Associated with Axillary Brachial Plexus Block: A case report
- Brachial Plexus Injury Following Axillary Brachial Plexus Block Using a Transarterial Approach: A case report
- Continuous Brachial Plexus Block as a Treatment for Intractable Pain Management of Malignancy Involving in Brachial Plexus: A report of 3 cases
- Steroid Injection into the Compartment of the Brachial Plexus in a Pediatric Patient with Traumatic Brachial Plexus Injury: A case report
