Korean Circ J.
2015 Nov;45(6):531-534. 10.4070/kcj.2015.45.6.531.
A Rare Cause of Secondary Hypertension in A Young Adult
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Dong-A University College of Medicine, Busan, Korea. thpark65@dau.ac.kr
- 2Department of Internal Medicine, Dong-A University College of Medicine, Busan, Korea.
- 3Department of Pathology, Dong-A University College of Medicine, Busan, Korea.
- 4Department of Cardiovascular Surgery, Dong-A University College of Medicine, Busan, Korea.
- KMID: 2223794
- DOI: http://doi.org/10.4070/kcj.2015.45.6.531
Abstract
- Reninoma is a rare, renin-secreting, benign renal neoplasm that can cause secondary hypertension. We report a case of a 21-year-old man who suffered from progressively worsening headache for 2 months with a history of hypertension for 7 years. Laboratory studies showed normal potassium level, increased basal plasma renin activity, and normal serum aldosterone level. Abdominal computed tomography and magnetic resonance imaging revealed a small mass in the middle region of the right kidney. Partial nephrectomy was performed; immunohistochemical results demonstrated typical features of reninoma. Postoperatively, blood pressure and potassium level were normal at the 2-month follow-up.
Keyword
MeSH Terms
Figure
-
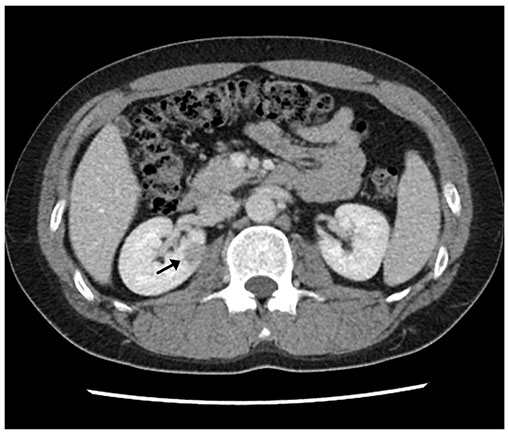
Fig. 1 Computed tomography scan shows a well-defined mass of 1.7×1 cm (arrow) in the middle portion of right kidney.
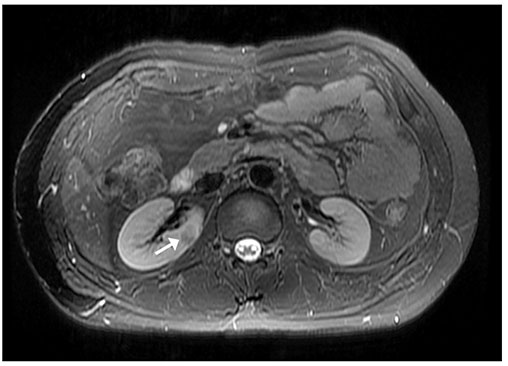
Fig. 2 T2-weighted magnetic resonance imaging shows a small solid mass (arrow) in the right kidney middle pole.
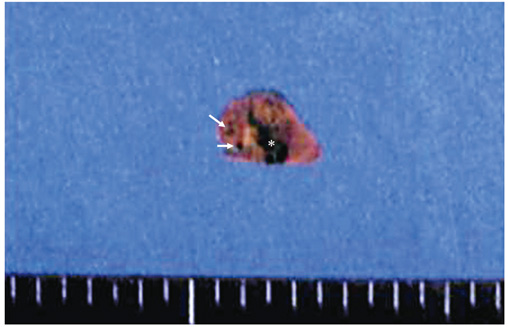
Fig. 3 Gross examination revealed a well-defined ovoid mass with foci of hemorrhage (star) and cystic changes (arrows).
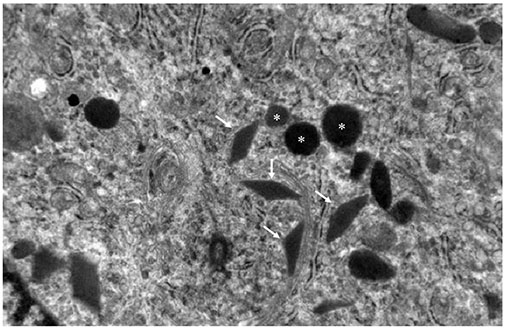
Fig. 4 Electron microscopy shows that tumor cells have typical rhomboid crystalline protogranules (stars) with electron dense bodies of different shapes (arrows).
Reference
-
1. Eddy RL, Sanchez SA. Renin-secreting renal neoplasm and hypertension with hypokalemia. Ann Intern Med. 1971; 75:725–729.2. Robertson PW, Klidjian A, Harding LK, Walters G, Lee MR, Robb-Smith AH. Hypertension due to a renin-secreting renal tumour. Am J Med. 1967; 43:963–976.3. Lin SY, Liu WY, Chen WC, Chen RH. Secondary hypertension due to a renin-secreting juxtaglomerular cell tumor. J Formos Med Assoc. 2010; 109:237–240.4. Wong L, Hsu TH, Perlroth MG, Hofmann LV, Haynes CM, Katznelson L. Reninoma: case report and literature review. J Hypertens. 2008; 26:368–373.5. Conn JW, Cohen EL, Lucas CP, et al. Primary reninism. Hypertension, hyperreninemia, and secondary aldosteronism due to renin-producing juxtaglomerular cell tumors. Arch Intern Med. 1972; 130:682–696.6. Dong D, Li H, Yan W, Xu W. Juxtaglomerular cell tumor of the kidney--a new classification scheme. Urol Oncol. 2010; 28:34–38.7. Dong D, Li H, Yan W, Xu W, Lu L, Zeng Z. The diagnosis and surgical management of juxtaglomerular cell tumor of the kidney. J Hypertens. 2010; 28:628–632.8. Lindop GB, Stewart JA, Downie TT. The immunocytochemical demonstration of renin in a juxtaglomerular cell tumour by light and electron microscopy. Histopathology. 1983; 7:421–431.9. Kim HJ, Kim CH, Choi YJ, Ayala AG, Amirikachi M, Ro JY. Juxtaglomerular cell tumor of kidney with CD34 and CD117 immunoreactivity: report of 5 cases. Arch Pathol Lab Med. 2006; 130:707–711.10. Mete UK, Niranjan J, Kusum J, Rajesh LS, Goswami AK, Sharma SK. Reninoma treated with nephron-sparing surgery. Urology. 2003; 61:1259.11. Haab F, Duclos JM, Guyenne T, Plouin PF, Corvol P. Renin secretng tumors: diagnosis, conservative surgical approach and long-term results. J Urol. 1995; 153:1781–1784.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute Myocardial Infarction Associated with Secondary Hypertension by Renal Juxtaglomerular Cell Tumor
- Diagnosis and Treatment of Secondary Hypertension
- The Experiences of Young Adult with Hypertension
- The Overview of Endocrine Hypertension
- Prevalene of Secondary Hypertension in Yeungnam University Hospital
