Two Cases of Superior Limbic Keratoconjunctivitis Treated with Bevacizumab and Triamcinolone Injection
- Affiliations
-
- 1Department of Ophthalmology, Chung-Ang University College of Medicine, Seoul, Korea. jck50ey@kornet.net
- KMID: 2218277
- DOI: http://doi.org/10.3341/jkos.2014.55.3.443
Abstract
- PURPOSE
To report two cases of intractable superior limbic keratoconjunctivitis (SLK) treated with bevacizumab and triamcinolone injection.
CASE SUMMARY
A 69-year-old female visited our clinic with pain in the left eye for 3 days and was diagnosed with SLK in her left eye. After 3 months of using steroid eye drops, artificial tears, and oral steroid intermittently, there was no improvement in symptoms and signs, thus this case was considered intractable with the conventional therapy. A mixture of bevacizumab (0.15 cc) and triamcinolone (0.05 cc) was injected into the sub-tenon's capsule of the left eye. After 1 week, all symptoms and signs disappeared, and there was no recurrence for 6 months. A 55-year-old female was transferred to our clinic due to SLK that did not respond to artificial tears, steroid eye drops, punctal occlusion, and botox injection for 3 months. A mixture of bevacizumab (0.15 cc) and triamcinolone (0.05 cc) was injected into the sub-tenon's capsule of the left eye. After 2 weeks, all symptoms and signs were improved, and there was no recurrence for 4 months.
CONCLUSIONS
The presented 2 SLK cases are meaningful, because neovascularization disappeared and controlled inflammation was obtained following sub-tenon injection with both bevacizumab and triamcinolone.
MeSH Terms
Figure
-
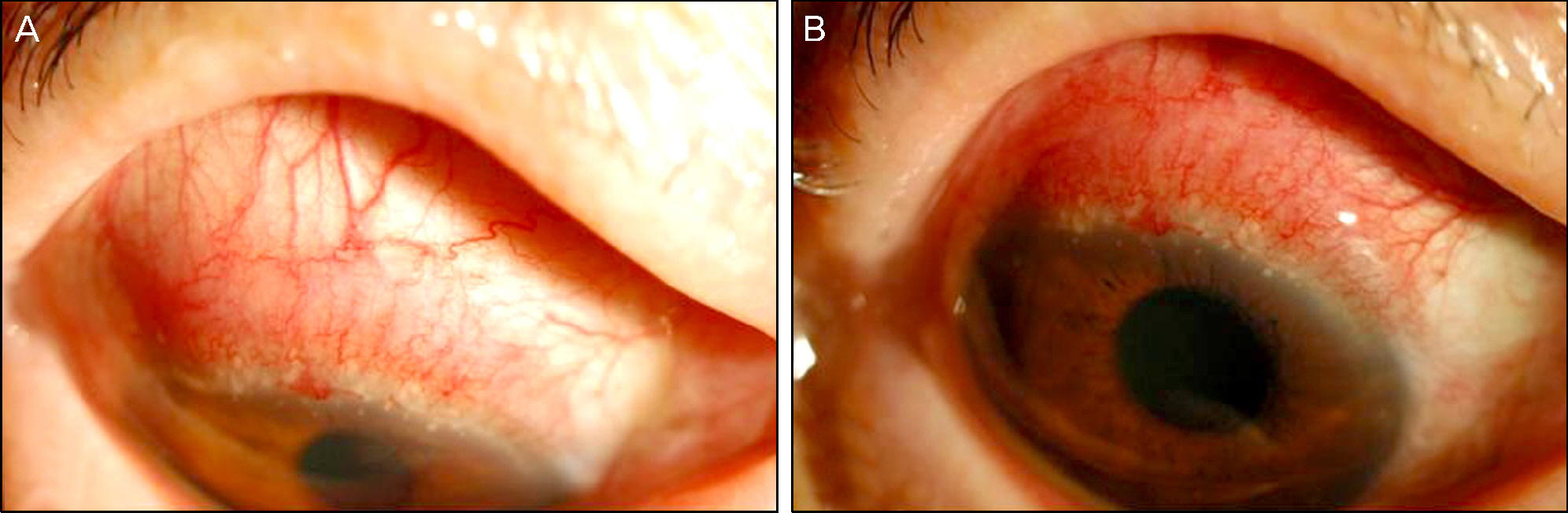
Figure 1. (A, B) Photographs of the left eye. A 69-years-old female visited with left eye pain. At initial visit, the superior limbus and superior limbic conjunctiva was diffusely stained by Rose Bengal along with injections and pannus in her left eye. She was diagnosed with the Superior limbic keratoconjunctivitis on the left eye.
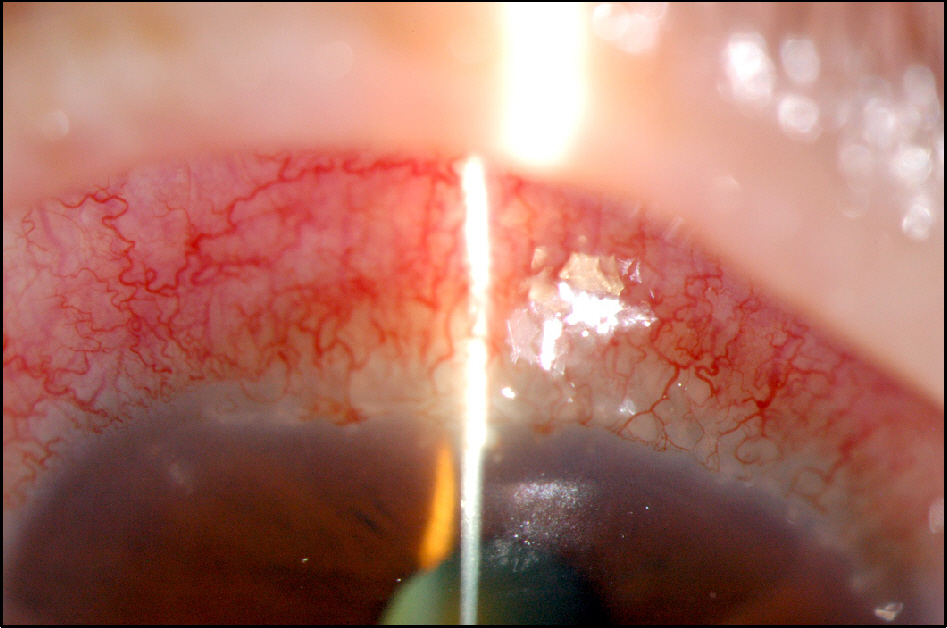
Figure 2. After 2 months treatment of eye drops (Cravit 4 times a day, Predforte 4 times a day) there was no symptom relief. Chronic inflammatory signs, neovascularization, and increased pannus was observed on her left eye.
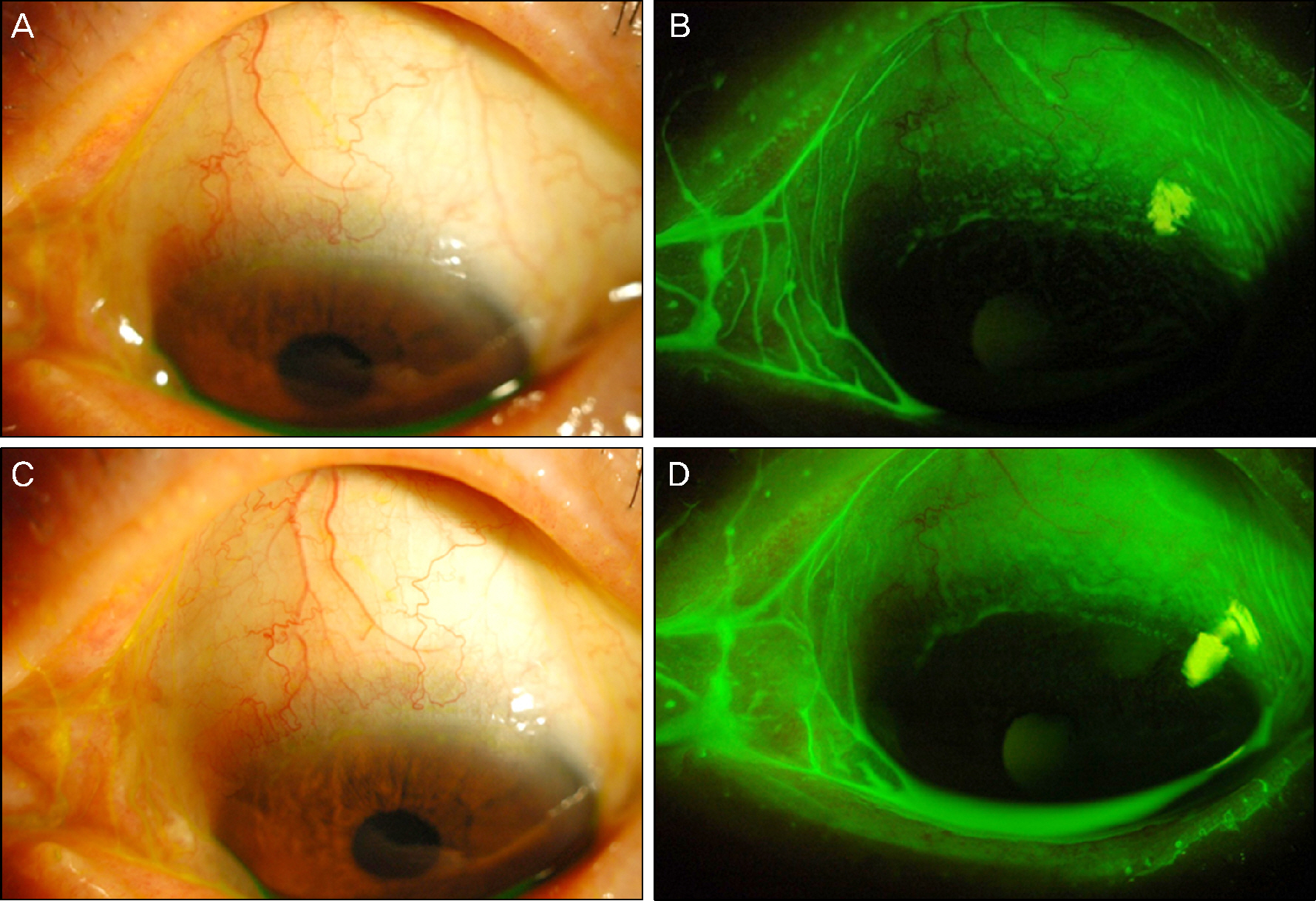
Figure 3. (A, B, C, D) Photographs of the left eye. After 1 week of bevacizumab (0.15 cc) and triamcinolone injection (0.05 cc) into the tenon capsule of the left eye, symptoms and signs including pain, injection, neovascularization, and diffuse fluorescein staining disappeared. The left eye had exhibited complete remission. (A, B) After 6 months, there was no recurrence (C, D).
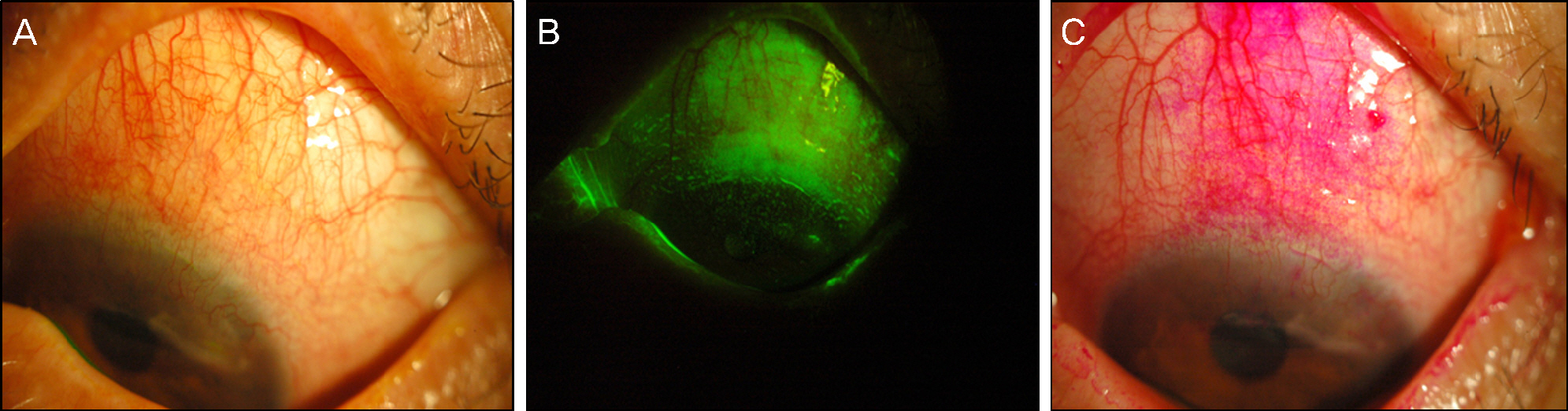
Figure 4. (A, B, C) Photographs of the left eye. A 55 years old female was transferred for intractable superior limbic keratoconjunctivitis. She had been treated with artificial tears, steroid eye drops, punctual occlusion, and botox injections for 3 months, but there was no symptom relief and no improvement on physical exams. At the initial visit the superior limbic conjunctiva was diffusely stained by fluorescein, Rose Bengal stain (B, C), along with injections and neovascularization in her left eye (A).
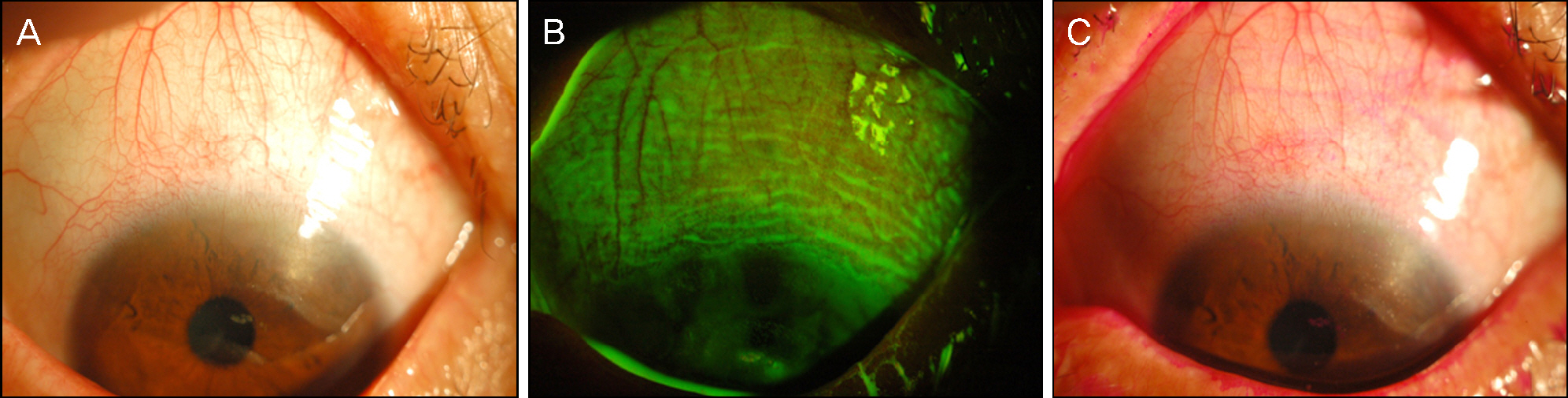
Figure 5. (A, B, C) Photographs of the left eye. After 2 weeks of bevacizumab (0.15 cc) and triamcinolone injection (0.05 cc) into the tenon capsule of the left eye pain, injection, neovascularization, and diffuse fluorescein and Rose Bengal staining disappeared.
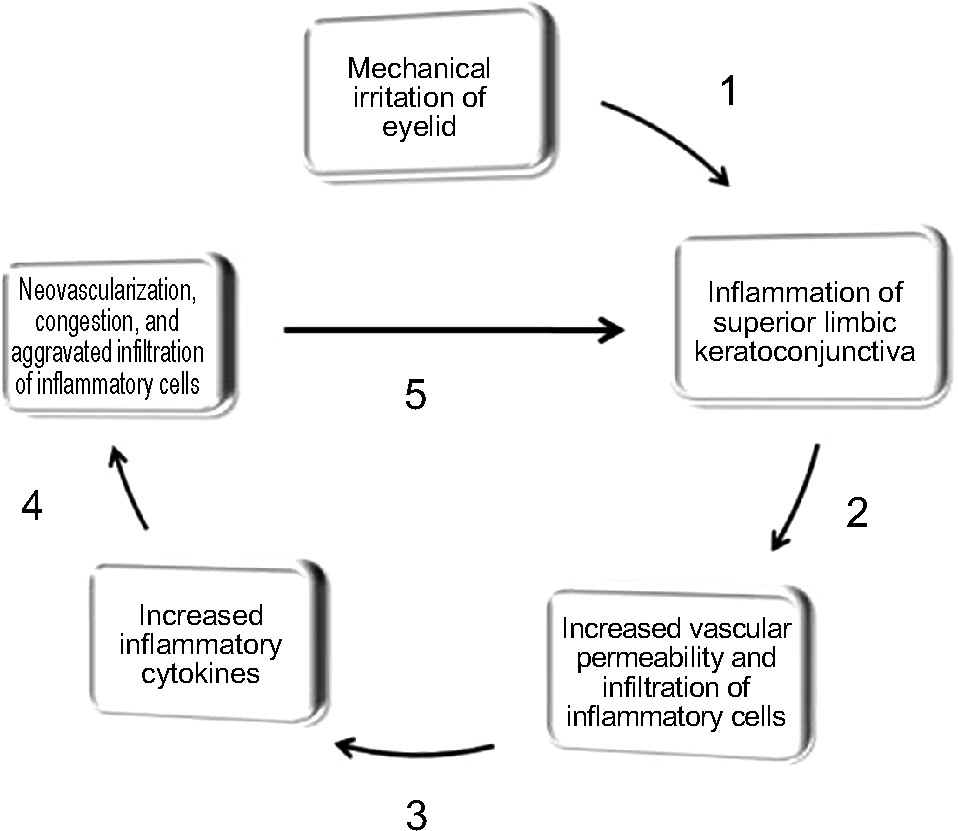
Figure 6. Proposed inflammatory cycle model of superior limbic keratoconjunctivitis.njunctivitis.
Reference
-
References
1. Nelson JD. Superior limbic keratoconjunctivitis (SLK). Eye (Londo). 1989; 3:180–9.
Article2. Confino J, Brown SI. Treatment of superior limbic keratoconjunctivitis with topical cromolyn sodium. Ann Ophthalmol. 1987; 19:129–31.3. Sahin A, Bozkurt B, Irekec M. Topical cyclosporine a in the treatment of superior limbic keratoconjunctivitis: a long-term fol-low-up. Cornea. 2008; 27:193–5.4. Chun YS, Kim JC. Treatment of superior limbic keratoconjunctivitis with a large-diameter contact lens and Botulium Toxin A. Cornea. 2009; 28:752–8.5. Shen YC, Wang CY, Tsai HY, Lee YF. Supratarsal triamcinolone injection in the treatment of superior limbic keratoconjunctivitis. Cornea. 2007; 26:423–6.
Article6. Yang HY, Fujishima H, Toda I, et al. Lacrimal punctal occlusion for the treatment of superior limbic keratoconjunctivitis. Am J Ophthalmol. 1997; 124:80–7.
Article7. Sun YC, Hsiao CH, Chen WL, et al. Conjunctival resection combined with tenon layer excision and the involvement of mast cells in superior limbic keratoconjunctivitis. Am J Ophthalmol. 2008; 145:445–52.
Article8. Udell IJ, Kenyon KR, Sawa M, Dohiman CH. Treatment of superior limbic keratoconjunctivitis by thermocauterization of the superior bulbar conjunctiva. Ophthalmol. 1986; 93:162–6.
Article9. Kojima T, Matsumoto Y, Ibrahim OM, et al. In vivo evaluation of superior limbic keratoconjunctivitis using laser scanning confocal microscopy and conjunctival impression cytology. Invest Ophthalmol Vis Sci. 2010; 51:3986–92.
Article10. Kadrmas EF, Bartley GB. Superior limbic keratoconjunctivitis. A prognostic sign for severe Gravesophthalmopathy. Ophthalmol. 1995; 102:1472–5.11. Matsuda A, Tagawa Y, Matsuda H. TGF-beta2, tenascin, and in-tegrin beta1 expression in superior limbic keratoconjunctivitis. Jpn J Ophthalmo. 1999; 43:251–6.12. Cher I. Superior limbic keratoconjunctivitis: multifactorial me-chanical pathogenesis. Clin Experiment Ophthalmol. 2000; 28:181–4.
Article13. Metcalfe DD, Baram D, Mekori YA. Mast cells. Physiol Rev. 1997; 77:1033–79.
Article14. Kojima T, Matsumoto Y, Ibrahim OM, et al. In vivo evaluation of superior limbic keratoconjunctivitis using laser scanning confocal microscopy and conjunctival impression cytology. Invest Ophthalmol Vis Sci. 2010; 51:3986–92.
Article15. Jackson JR, Seed MP, Kircher CH, et al. The codependence of an-giogenesis and chronic inflammation. FASEB J. 1997; 11:457–65.
Article16. Ferrara N, Hillan KJ, Gerber HP, Novotny W. Discovery and development of bevacizumab, an anti-VEGF antibody for treating cancer. Nat Rev Drug Discov. 2004; 3:391–400.
Article17. Nakao S, Zandi S, Lara-Castillo N, et al. Larger therapeutic win-dow for steroid versus VEGF-A inhibitor in inflammatory angio-genesis: surprisingly similar impact on leukocyte infiltration. Invest Ophthalmol Vis Sci. 2012; 53:3296–302.
Article18. Oh JY, Kim MK, Shin MS, et al. The anti-inflammatory effect of subconjunctival bevacizumab on chemically burned rat corneas. Curr Eye Res. 2009; 34:85–91.
Article19. Wershil BK, Furuta GT, Lavigne JA, et al. Dexamethasone and cyclosporin A suppress mast cell-leukocyte cytokine cascades by multiple echanisms. Int Arch Allergy Immunol. 1995; 107:323–4.20. Itakura H, Akiyama H, Hagimura N, et al. Triamcinolone acetonide suppresses interleukin-1 beta-mediated increase in vascular endothelial growth factor expression in cultured rat Muller cells. Graefes Arch Clin Exp Ophthalmol. 2006; 244:226–31.21. Ferrante P, Ramsey A, Bunce C, Lightman S. Clinical trial to compare efficacy and side-effects of injection of posterior sub-Tenon triaet al. mcinolone versus orbital floor methylprednisolone in the management of posterior uveitis. Clin Exp Ophthalmol. 2004; 32:563–8.22. You IC, Kang IS, Lee SH, Yoon KC. Therapeutic effect of subconjunctival injection of bevacizumab in the treatment of corneal neovascularization. Acta Ophthalmol. 2009; 87:653–8.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Superior Limbic Keratoconjunctivits
- A Case of Conjunctival Lithiasis with Clinical Manifestations of Superior Limbic Keratoconjunctivitis
- A Case of Conjunctival Lymphangioma With Clinical Manifestations of Superior Limbic Keratoconjunctivitis After Upper Lid Blepharoplasty
- The Effect of Intravitreal Triamcinolone Acetonide and Bevacizumab Injection on Intraocular Pressure
- Comparison of Intravitreal Bevacizumab Alone Injection and Intravitreal Combination Low-Dose Bevacizumab-Triamcinolone Injection or Diabetic Macular Edema
