The Minimal Postoperative Follow-Up Period to Determine Secondary Surgery in Patients with Intermittent Exotropia
- Affiliations
-
- 1Department of Ophthalmology, Gachon University Gil Hospital, Incheon, Korea. hjpaik@gilhospital.com
- KMID: 2218092
- DOI: http://doi.org/10.3341/jkos.2014.55.5.711
Abstract
- PURPOSE
We investigated the recommended minimum postoperative follow-up period for the determination of secondary corrective surgery for the consecutive esotropia (ET) and recurrent exotropia (XT) after the first intermittent XT surgery.
METHODS
The medical records of 728 patients who underwent surgical treatment for intermittent XT between 2004 and 2009 with a minimum postoperative follow-up of 1 year were retrospectively reviewed. Each patient underwent a detailed sensory and motor examination, including measurements of near and distance stereoacuity, alternating-cover test, and extraocular muscle function testing. Consecutive ET was defined as esodeviation over 15 prism diopter (PD) at distance persisting for more than 6 months after surgery despite medical treatment. Recurrent XT was defined as exodeviation over 15 PD at distance after surgery despite medical treatment.
RESULTS
The mean age of the 728 patients at first surgery was 7.5 years (range, 22 months - 30 years). When only the motor outcome was considered, 663 patients (91.1%) had an orthrotropia at the final follow-up and 44 patients (6.0%) among consecutive ET patients and 21 patients (2.9%) who had a recurrent XT underwent secondary surgical correction. Binocularity decreased postoperatively in patients with consecutive ET (p < 0.001), whereas the other patients demonstrated improved stereopsis postoperatively (p = 0.041, 0.021). Patients with consecutive ET showed esodeviation over 10 PD when compared with orthotropia after 2 months postoperatively (p = 0.005). At 6 months postoperatively, 17 (81.0%) of 21 patients with recurrent XT showed orthotropia with an exodeviation over 11 PD after 18 months postoperatively.
CONCLUSIONS
The success rate of surgical correction for intermittent XT showed a favorable outcome. However, careful concern for consecutive ET and recurrent XT are required in postoperative follow-up periods. Over-corrected or consecutive ETs need early surgical correction because no further improvement of ocular alignment will occur after 2 months postoperatively and delayed correction can result in poor sensory binocularity. Under-corrected or recurrent XT should be observed for an extended period because of the exotropic drift after surgery, thus requiring periodic long term follow-up for secondary surgery at least for 18 months postoperatively.
Keyword
MeSH Terms
Figure
-
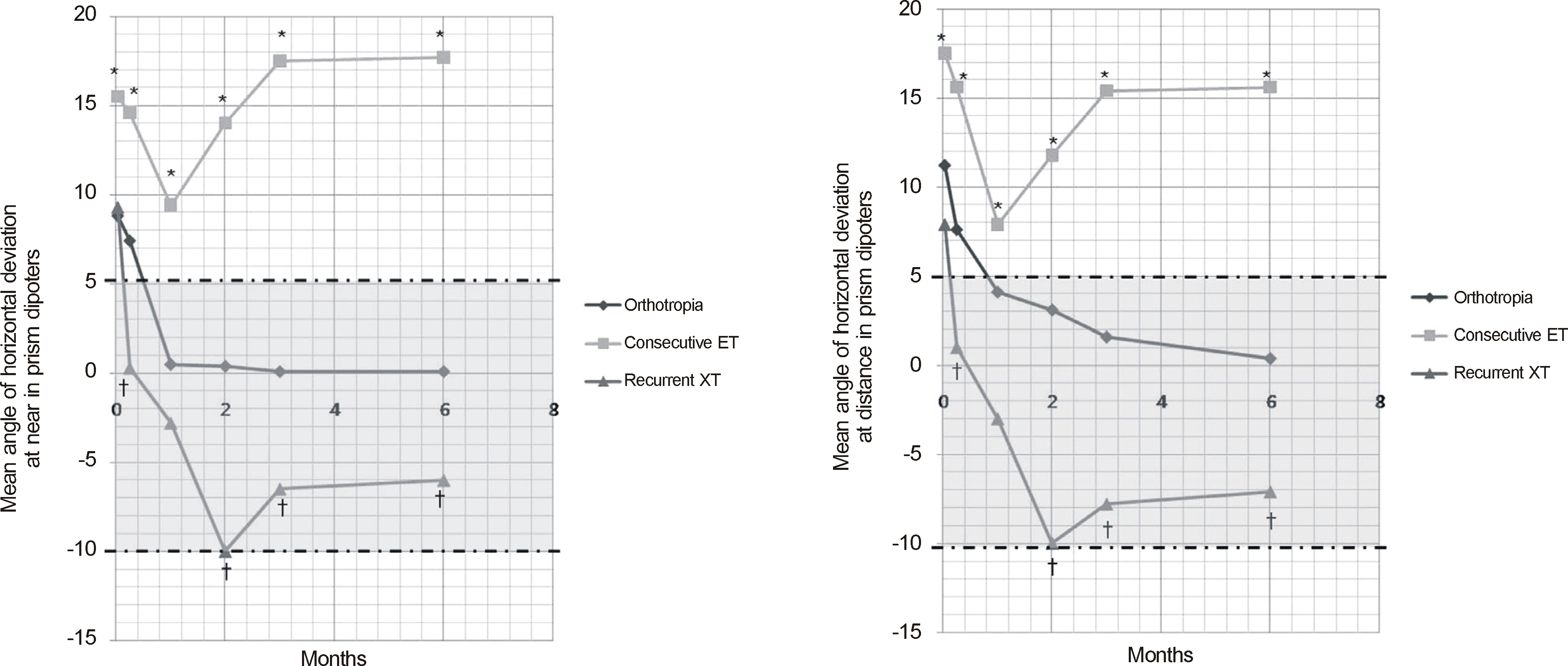
Figure 1. Postoperative deviation after first surgery among “Consecutive ET”,“Orthotropia”, and “Recurrent XT”. ET = esotropia; XT = exotropia. *,†Statistically significant different.
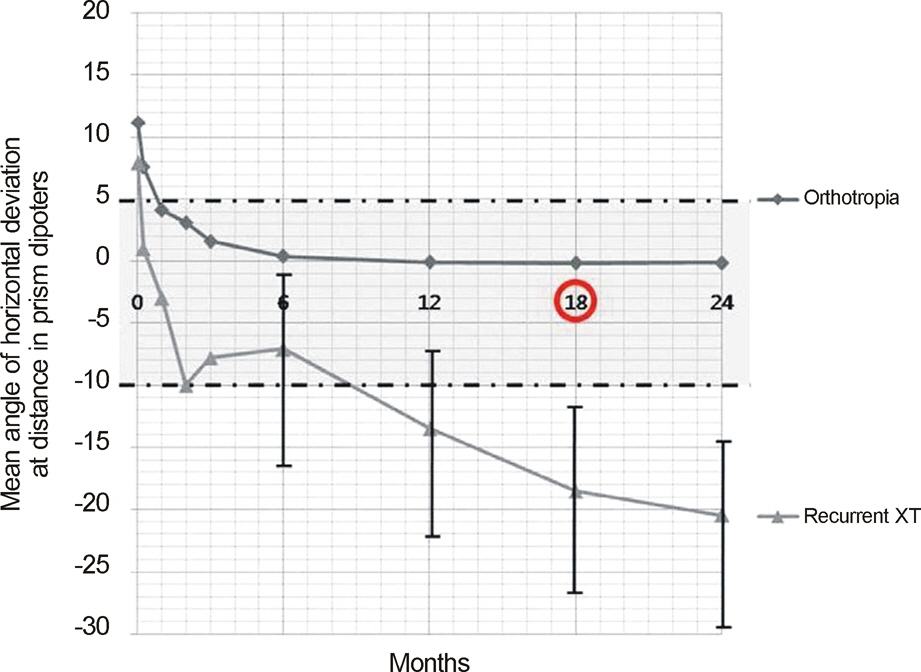
Figure 2. Postoperative deviation at distance after first surgery between “Orthotropia” and “Recurrent XT”. XT = exotropia.
Cited by 4 articles
-
Changes in Types of Recurrent Intermittent Exotropia after Surgical Correction of Basic Type Intermittent Exotropia
Sung Ha Hwang, Hae Jung Paik
J Korean Ophthalmol Soc. 2018;59(8):760-765. doi: 10.3341/jkos.2018.59.8.760.Characteristics of Patients Who Are Not Responsive to Alternate Patching for Overcorrected Intermittent Exotropia
Jung Yup Kim, Hae Rang Kim, Soo Jung Lee
Korean J Ophthalmol. 2018;32(4):319-327. doi: 10.3341/kjo.2017.0086.The Effect of Alternating Occlusion Therapy in Patients with Early Recurrence after Intermittent Exotropia Surgery
Sang Yoon Hyun, Mi Young Choi
J Korean Ophthalmol Soc. 2016;57(4):623-627. doi: 10.3341/jkos.2016.57.4.623.Changes in the Effects of Bilateral Lateral Rectus Muscle Recession According to Preoperative Angle Deviation
Sung Ha Hwang, Hae Jung Paik
J Korean Ophthalmol Soc. 2020;61(3):281-287. doi: 10.3341/jkos.2020.61.3.281.
Reference
-
References
1. Yu YS, Kim SM, Kwon JY, et al. Preschool vision screening in Korea; Preliminary study. J Korean Ophthalmol Soc. 1991; 32:1092–6.2. Lee SN, Rhee KO, Kim CS, Lee TY. Five-year follow-up of re-fractive error and visual acuity in preschool children. J Korean Opthalmol Soc. 2004; 45:1336–47.3. Figueira EC, Hing S. Intermittent exotropia: comparison of treatments. Clin Experiment Ophthalmol. 2006; 34:245–51.
Article4. Park JY, Sohn HY, Cho YA. Is the non surgical treatment effective on intermittent exotropia in children school-age. J Korean Ophthalmol Soc. 1995; 36:1561–7.5. Raab EL, Parks MM. Recession of the lateral recti. Early and late postoperative alignments. Arch Ophthalmol. 1969; 82:203–8.6. Scott WE, Keech R, March AJ. The postoperative results and stability of exodeviations. Arch Ophthalmol. 1981; 99:1814–8.
Article7. Keech RV, Stewart SA. The surgical overcorrection of intermittent exotropia. J Pediatr Ophthalmol Strabismus. 1990; 27:218–20.
Article8. Hardesty HH. Treatment of overcorrected intermittent exotropia. Am J Ophthalmol. 1968; 66:80–6.
Article9. Jung SH, Rah SH. The clinical course of consecutive esotropia after surgical correction. Korean J Ophthalmol. 2007; 21:228–31.
Article10. Hahm IR, Yoon SW, Baek SH, Kong SM. The clinical course of recurrent exotropia after reoperation for exodeviation. Korean J Ophthalmol. 2005; 19:140–4.
Article11. Oh JY, Hwang JM. Survival analysis of365 patients with exotropia after surgery. Eye (Lond). 2006; 20:1268–72.12. Clarke WN, Noel LP. Surgical results in intermittent exotropia. Can J Ophthalmol. 1981; 16:66–9.13. Maruo T, Kubota N, Sakaue T, Usui C. Intermittent exotropia surgery in children: long term outcome regarding changes in binocular alignment. A Study of 666 Cases. Binocul Vis Strabismus Q. 2001; 16:265–70.14. Park JL, Son MH, Yun IH, Won IG. The clinical analysis of surgical methods in intermittent exotropia. J Korean Ophthalmol Soc. 2002; 43:526–32.15. Zibrandtsen P, Rindziunski E, Gregersen E. Ten years follow-up of surgery for intermittent exotropia. Acta Ophthalmol (Copenh). 1986; 64:374–8.
Article16. Baker JD. Twenty-year follow-up of surgery for intermittent exotropia. J AAPOS. 2008; 12:227–32.
Article17. Chia A, Seenyen L, Long QB. Surgical experiences with two-muscle surgery for the treatment of intermittent exotropia. J AAPOS. 2006; 10:206–11.
Article18. Jeoung JW, Lee MJ, Hwang JM. Bilateral lateral rectus recession versus unilateral recess-resect procedure for exotropia with a dominant eye. Am J Ophthalmol. 2006; 141:683–8.
Article19. Ekdawi NS, Nusz KJ, Diehl NN, Mohney BG. Postoperative outcomes in children with intermittent exotropia from a population-based cohort. J AAPOS. 2009; 13:4–7.
Article20. Pineles SL, Ela-Dalman N, Zvansky AG, et al. Long-term results of the surgical management of intermittent exotropia. J AAPOS. 2010; 14:298–304.
Article21. Parks MM, Mirchell P. Concomittant exodeviations. In : Duane TD, editor. Clinical Ophthalmology. 1. Philadelphia: JB Lippincott;1988. p. p1.22. Burian HM. Exodeviation: Their classification, diagnosis and treatment. Am J Ophthalmol. 1966; 62:1161–6.23. Ruttum MS. Initial versus subsequent postoperative motor alignment in intermittent exotropia. J AAPOS. 1997; 1:88–91.
Article24. Gezer A, Sezen F, Nasri N, Gozum N. Factors influencing the outcome of strabismus surgery in patient with exotropia. J AAPOS. 2004; 8:56–60.25. Knapp P, Helveston EM, Jampolsky A, et al. Transections of the New Orleans Academy of Ophthalmology. Symposium on Strabismus. St Louis: C.V. Mosby;1971. p. 233–41.26. Roh JH, Paik HJ. Clinical study on factors associated with recurrence and reoperation in intermittent exotropia. J Korean Ophthalmol Soc. 2008; 49:1114–9.
Article27. von Noorden GK, Campos EC. Exodeviation. Binocular vision and ocular motility: therapy and management of strabismus. 6th ed.St Louis: CV Mosby;2002. chap. 17.28. Hardesty HH, Boynton JR, Keenan JP. Treatment of intermittent exotropia. Arch Ophthalmol. 1978; 96:268–74.
Article29. Cho YA, Kang SM, Roh GH. Asymmetric Bilateral Lateral Recti Recession in Intermittent Exotropia. J Korean Ophthalmol Soc. 1999; 40:544–9.30. Shin YJ, Chang BL. The clinical outcome of the consecutive esotropia after surgical correction. J Korean Ophthalmol Soc. 2003; 44:2085–90.31. Elsas FJ. Consecutive Esotropia. Am Orthopt J. 1992; 42:94–7.
Article32. Jampolsky A. Surgical correction of overcorrection in strabismus. Am Orthopt J. 1976; 26:14–9.33. Son AN, Park SC, Lee WR. Clinical study of consecutive esotropia. J Korean Ophthalmol Soc. 1990; 31:1328–34.34. Park HS, Kim JB, Seo MS, Park YG. A study on the consecutive esotropia after intermittent exotropia surgery. J Korean Ophthalmol Soc. 1994; 35:1327–34.35. Kim SJ, Lee SH, Woo KH. The surgical correction of consecutive esotropia. J Korean Ophthalmol Soc. 1994; 35:332–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Surgical Outcome of Intermittent Exotropia and the Prognostic Factors
- The Clinical Course of Recurrent Intermittent Exotropia After Previous Unilateral Recess-Resection Surgery
- Unilateral Recession-Resection Versus Re-resection of Medial Rectus in Recurrent Intermittent Exotropia
- The Effect of Unilateral Medial Rectus Resection for Recurrent Intermittent Exotropia
- The influence of fusional divergence on the surgical results in intermittent exotropia
