J Korean Ophthalmol Soc.
2013 Jan;54(1):117-122. 10.3341/jkos.2013.54.1.117.
Additional Retrobulbar Triamcinolone Acetonide Injection for Retrobulbar Optic Neuritis Patients
- Affiliations
-
- 1Department of Ophthalmology, Kyungpook National University School of Medicine, Daegu, Korea. byjun424@hotmail.com
- KMID: 2216459
- DOI: http://doi.org/10.3341/jkos.2013.54.1.117
Abstract
- PURPOSE
To evaluate the effect of additional retrobulbar triamcinolone acetonide (TA) injection on early recovery of visual acuity in retrobulbar optic neuritis patients.
METHODS
A prospective, randomized clinical study including 30 patients with retrobulbar optic neuritis was conducted between March 2003 and June 2007. Patients were divided into 2 groups: Group 1 (n = 9) with retrobulbar triamcinolone (TA, 40 mg/1 ml) injection on the first day of ONTT protocol, and group 2 (n = 21) with conventional ONTT protocol. The following parameters were measured and analyzed: patient's sex, age, pupillary reactions, color vision, visual field, and best-corrected visual acuity before treatment, and after 1 day, 1 week, 2 weeks, 1 month, and 3 months of follow-up.
RESULTS
Mean visual acuity before treatment was 1.00 +/- 0.89 log MAR units in group 1 and 0.98 +/- 0.75 log MAR units in group 2. One day after injection, visual acuity was better in group 1 (0.50 +/- 0.42 log MAR units) than in group 2 (0.73 +/- 0.61 log MAR units), however, there was no statistically significant difference between the 2 groups (p = 0.07). There was no significant difference in visual acuity, recovery of RAPD, color vision, or visual field at 3 months of follow-up. No serious side effect related to retrobulbar TA injection was observed.
CONCLUSIONS
Additional retrobulbar TA injection may help optic neuritis patients who have a need for prompt visual recovery. However, further studies are required to ascertain whether this procedure can help early recovery of visual acuity in retrobulbar optic neuritis patients.
Keyword
MeSH Terms
Figure
-
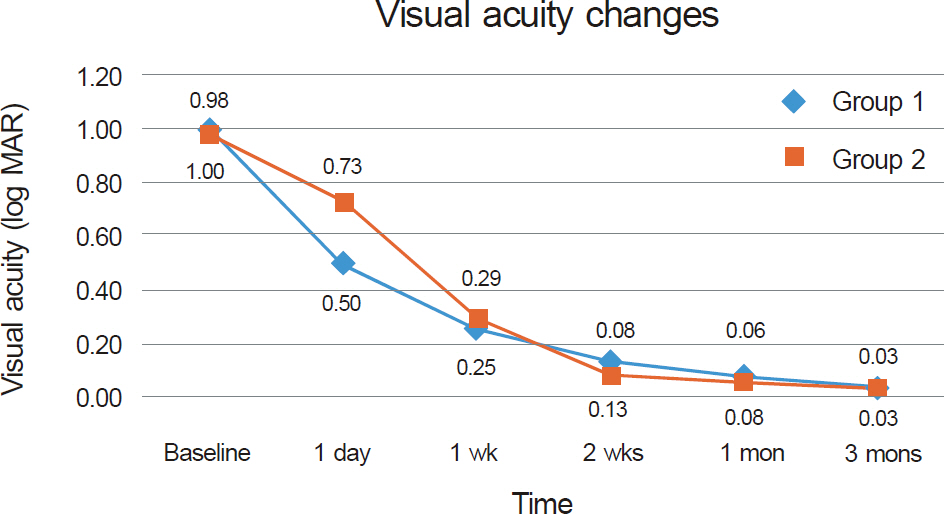
Figure 1. Mean BCVA before treatment and after 1 day, 1 week, 2 weeks, 1 month, and 3 months of follow-up.
Reference
-
References
1. Ebers GC. Optic neuritis and multiple sclerosis. Arch Neurol. 1985; 42:702–4.
Article2. Rizzo JF 3rd, Lessell S. Risk of developing multiple sclerosis after uncomplicated optic neuritis: a long-term prospective study. Neurology. 1988; 38:185–90.3. Optic Neuritis Study Group. Multiple sclerosis risk after optic abdominal: final optic neuritis treatment trial follow-up. Arch Neurol. 2008; 65:727–32.4. Foroozan R, Buono LM, Savino PJ, Sergott RC. Acute demyelinating optic neuritis. Curr Opin Ophthalmol. 2002; 13:375–80.
Article5. Lee YJ, Chang BL. Clinical manifestations of optic neuritis. J Korean Ophthalmol Soc. 1997; 38:1969–74.6. Volpe NJ. Optic neuritis: historical aspects. J Neuroophthalmol. 2001; 21:302–9.
Article7. Beck RW, Cleary PA, Anderson MM Jr, et al. A randomized, abdominalled trial of corticosteroids in the treatment of acute optic neuritis. The Optic Neuritis Study Group. N Engl J Med. 1992; 326:581–8.8. Optic Neuritis Study Group. Visual function 15 years after optic neuritis: a final follow-up report from the Optic Neuritis Treatment Trial. Ophthalmology. 2008; 115:1079–82.9. Beck RW, Gal RL. Treatment of acute optic neuritis: a summary of findings from the optic neuritis treatment trial. Arch Ophthalmol. 2008; 126:994–5.10. Volpe NJ. The optic neuritis treatment trial: a definitive answer and profound impact with unexpected results. Arch Ophthalmol. 2008; 126:996–9.11. Keltner JL, Johnson CA, Spurr JO, Beck RW. Visual field profile of optic neuritis. One-year follow-up in the Optic Neuritis Treatment Trial. Arch Ophthalmol. 1994; 112:946–53.
Article12. Lincoff HA, Kreissig I, Lincoff N, et al. Elevated concentration of intraocular cortisol obtained by sequential parabulbar injection in rabbit model. Klin Monbl Augenheilkd. 2001; 218:445–50.13. Gould ES, Bird AC, Leaver PK, McDonald WI. Treatmenf of optic neuritis by retrobulbar injection of triamcinolone. Br Med J. 1977; 1:1495–7.
Article14. Feldman-Billard S, Lissak B, Kassaei R, et al. abdominal tolerance of pulse methylprednisolone therapy in patients with diabetes mellitus. Ophthalmology. 2005; 112:511–5.15. Kim JY, Ahn M. Side effects of intravenous methylprednisolone pulse therapy in eye diseases. J Korean Ophthalmol Soc. 2008; 49:14–8.
Article16. Schindler RH, Chandler D, Thresher R, Machemer R. The abdominal of intravitreal triamcinolone acetonide. Am J Ophthalmol. 1982; 93:415–7.17. Bakri SJ, Beer PM. The effect of intravitreal triamcinolone abdominal on intraocular pressure. Ophthalmic Surg Lasers Imaging. 2003; 34:386–90.18. Gillies MC, Simpson JM, Billson FA, et al. Safety of an intravitreal injection of triamcinolone: results from a randomized clinical trial. Arch Ophthalmol. 2004; 122:336–40.19. Moshfeghi DM, Kaiser PK, Scott IU, et al. Acute endophthalmitis following intravitreal triamcinolone acetonide injection. Am J Ophthalmol. 2003; 136:791–6.
Article20. Roth DB, Chieh J, Spirn MJ, et al. Noninfectious endophthalmitis associated with intravitreal triamcinolone injection. Arch Ophthalmol. 2003; 121:1279–82.
Article21. Jonas JB, Söfker A, Degenring R. Intravitreal triamcinolone abdominal as an additional tool in pars plana vitrectomy for proliferative diabetic retinopathy. Eur J Ophthalmol. 2003; 13:468–73.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Optic Nerve Decompression in a Patient with Retrobulbar Neuritis Secondary to Paranasal Sinusitis
- Retrobulbar Optic Neuritis after COVID-19 Infection
- Clinical Characteristics of Optic Neuritis according to the Presence of Abnormal MRI Lesions
- Ret robulbar Optic Neuritis Associated with Multiple Sclerosis: Two Cases
- Central Retinal Artery Occlusion Without Retrobular Hemorrhage after Retrobulbar Anesthesia
