A Case of Congenital Monocular Elevation Deficiency Associated with Inferior Rectus Anomaly
- Affiliations
-
- 1Department of Ophthalmology, Bucheon St. Mary's Hospital, The Catholic University of Korea College of Medicine, Bucheon, Korea. nyeokang@catholic.ac.kr
- KMID: 2216410
- DOI: http://doi.org/10.3341/jkos.2012.53.12.1904
Abstract
- PURPOSE
To report a congenital monocular elevation deficiency (MED) associated with inferior rectus anomaly.
CASE SUMMARY
A 3-year-old, otherwise healthy boy presented with left hypotropia. He showed chin-up and left head turn with left pseudoptosis. On examination, there was a left hypertropia of 60 prism diopters (PD) and esotropia in primary position. Upgaze -4 limitation in abduction and -3 from primary position, poor Bell's phenomenon, and normal vertical saccadic velocity until midline were observed. On orbital CT, thin and nasally displaced left inferior rectus showing enlargement at its posterior segments near the orbital apex was observed. Forced duction test at surgery revealed a strong positive restriction and thin, taut, fibrotic inferior rectus was inserted and displaced nasally.
CONCLUSIONS
Left inferior rectus recession of 5.5 mm with 2.0 mm of temporal transposition improved elevation deficiency, but consecutive exotropia and hypotropia remained. Knapp procedure combined with left lateral rectus recession of 5.5 mm and left medial rectus resection of 4.5 mm, and right superior rectus recession of 9.5 mm were additionally performed. Pseudoptosis and chin elevation resolved but left hypotropia 10PD, and exotropia 6PD remained. Elevation restriction in primary position and abduction were improved but still persisted. This case indicated that MED may accompany congenital inferior rectus anomaly. If severe inferior rectus restriction is observed during the forced duction test, a structural anomaly of the inferior rectus causing motility defects of MED.
Figure
-
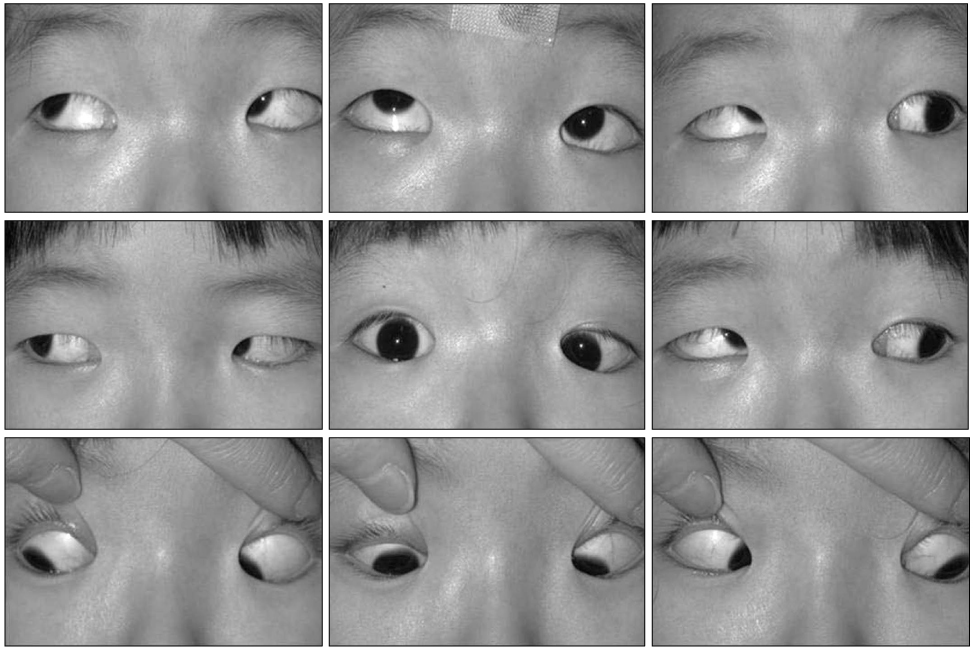
Figure 1 Preoperative ocular versions showing limited elevation on abduction and primary position in the left eye. Near- normal left inferior oblique rotation can be seen. Note accompanying deep epicanthal fold and pseudoptosis of the left eyelids.
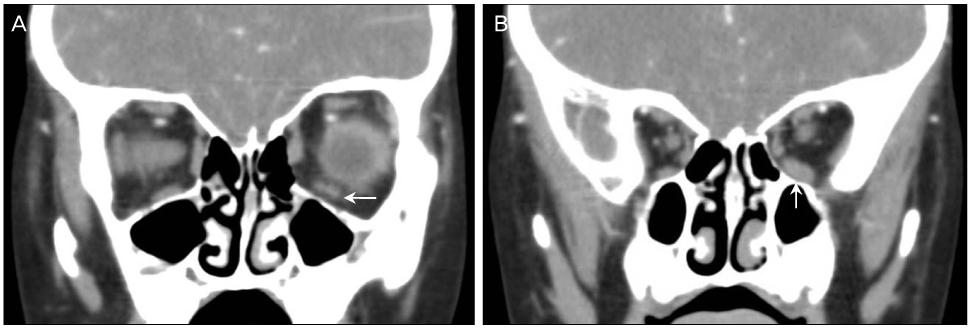
Figure 2 Coronal orbital CT showing thickening of the left inferior rectus muscle (arrow) compared to the right inferior rectus muscle near the orbital apex area.

Figure 3 Intraoperative findings showing nasally translating left inferior rectus muscle (white lines). The muscle hook is trying to pull the stiff and fibrotic inferior rectus muscle to the midline position.
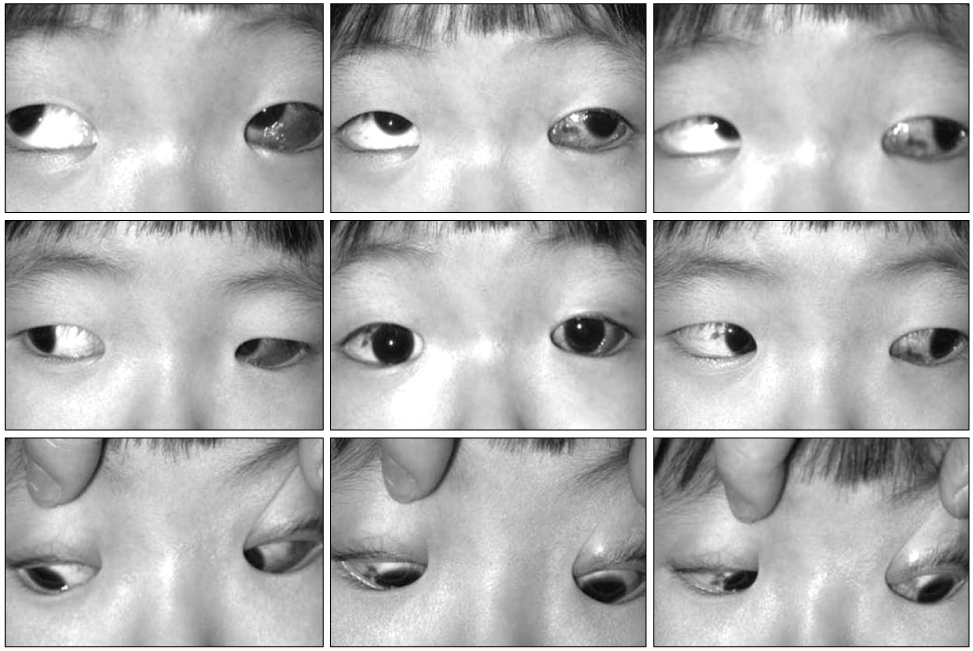
Figure 4 Ocular versions 1week after inferior rectus muscle recession showing improvement of upgaze in the primary position and abduction. But exotropia in the primary position and limitation of infraduction developed.
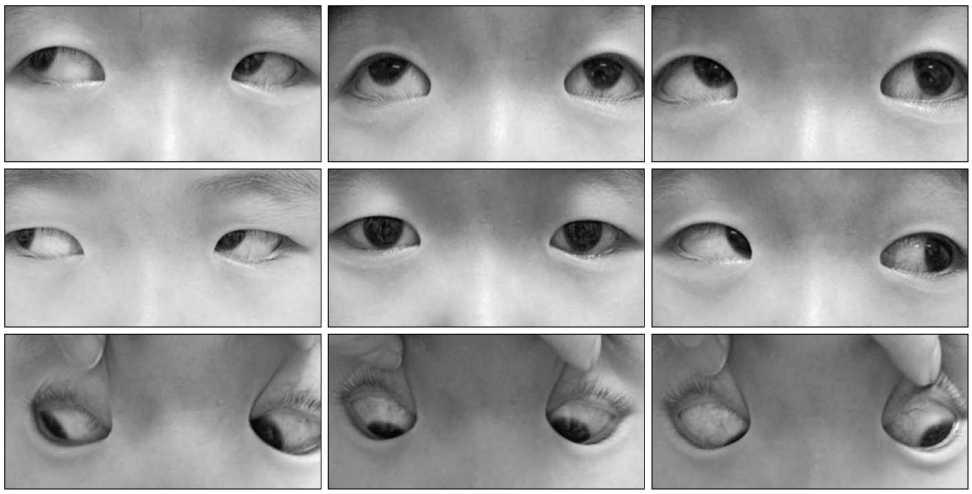
Figure 5 Ocular versions after Knapp procedure and right superior rectus recession. Upgaze limitation on primary position and abduction is improved but left hypotropia and downgaze limitation of the left eye remained.
Reference
-
1. Scott WE, Jackson OB. Double elevator palsy: the significance of inferior rectus restriction. Am Orthopt J. 1977. 27:5–10.2. Metz HS. Double elevator palsy. J Pediatr Ophthalmol Strabismus. 1981. 18:31–35.3. Ziffer AJ, Rosenbaum AL, Demer JL, Yee RD. Congenital double elevator palsy: vertical saccadic velocity utilizing the scleral search coil technique. J Pediatr Ophthalmol Strabismus. 1992. 29:142–149.4. Mims JL 3rd. "Double elevator" palsy eye supraducts during stage II general anesthesia supporting hypothesis of (supra) nuclear etiology. Binocul Vis Strabismus Q. 2005. 20:199–204.5. White JW. Paralysis of the superior rectus and the inferior oblique muscle of the same eye. Arch Ophthalmol. 1942. 27:366–371.6. Choi SY, Yoon IR, Won IG. 4 Cases of double elevator palsy. J Korean Ophthalmol Soc. 1991. 32:910–917.7. Lee SY, Kim KS. A case of double elevator palsy associated with blepharoptosis. J Korean Ophthalmol Soc. 1995. 36:1582–1587.8. Knapp P. The surgical treatment of double elevator paralysis. Trans Am Ophthalmol Soc. 1969. 67:304–323.9. Burke JP, Ruben JB, Scott WE. Vertical transposition of the horizontal recti (Knapp procedure) for the treatment of double elevator palsy: effectiveness and long-term stability. Br J Ophthalmol. 1992. 76:734–737.10. Snir M, Friling R, Kalish-Stiebel H, et al. Combined rectus muscle transposition with posterior fixation sutures for the treatment of double-elevator palsy. Ophthalmology. 2005. 112:933–938.11. Mcneer KW, Jampolsky A. Double elevator palsy caused by anomalous insertion of the inferior rectus. Am J Ophthalmol. 1965. 59:317–319.12. Paolillo RD, Burch PG, Torchia RT. Infantile contracture of inferior rectus muscle with resultant mechanical hypotropia. Am J Ophthalmol. 1969. 68:1057–1060.13. Prieto-Diaz J, Souza-Dias C. Strabismus. c2000. 4th ed. Boston: Butterworth-Heinemann;393–396.14. Maruo T, Kubota N, Sakaue T, et al. Outcome of surgery for congenital fibrosis of the inferior rectus muscle. Binocul Vis Strabismus Q. 2001. 16:105–110.15. Ford CS, Schwartze GM, Weaver RG, Troost BT. Monocular elevation paresis caused by ipsilateral lesion. Neurology. 1984. 34:1264–1267.16. Metz HS. Double elevator palsy. Arch Ophthalmol. 1979. 97:901–903.17. Dickey CF. Clinical presentation of congenital fibrosis and double elevator palsy. (Abstract). Am Orthopt J. 1993. 43:40–41.18. Prieto-Diaz J, Souza-Dias C. Strabismus. c2000. 4th ed. Boston: Butterworth-Heinermann;335.19. Lin Q, Man F, Wang N, et al. Diagnosis and surgical treatment of unilateral restrictive hypotropia and esotropia. J AAPOS. 2011. 15:5–8.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Use of the Levator Muscle as a Frontalis Sling in Monocular Elevation Deficiency
- Anomaly of Deep Inferior Epigastric Vessels detected at the Elevation of Rectus Abdominis Musculocutaneous Flap: A Case Report
- A Case of Double Elevator Palsy Associated with Blepharoptosis
- Two Cases of Congenital Fibrosis of the Extraocular Muleles
- Scleral Perforation During Inferior Rectus Muscle Recession in Congenital Fibrosis of the Extraocular Muscles
