J Korean Ophthalmol Soc.
2011 Mar;52(3):359-363. 10.3341/jkos.2011.52.3.359.
Delayed-Onset Expulsive Suprachoroidal Hemorrhage Due to a Trauma after Removal of Penetrating Keratoplasty Suture
- Affiliations
-
- 1Department of Ophthalmology, Soonchunhyang University College of Medicine, Seoul, Korea.
- 2Department of Ophthalmology, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. greenizy@lycos.co.kr
- KMID: 2214303
- DOI: http://doi.org/10.3341/jkos.2011.52.3.359
Abstract
- PURPOSE
To report a case of delayed-onset expulsive suprachoroidal hemorrhage due to trauma after removal of a penetrating keratoplasty suture.
CASE SUMMARY
A 66-year-old man had penetrating keratoplasty for bullous keratopathy performed in his left eye. After 1 year, the continuous suture was removed for adjustment of astigmatism. Four days after removal of the suture, the patient struck his left eye with the back of his hand, although at the time of injury he had no specific symptoms. Two days later, the patient noticed abrupt pain, decreased visual acuity, and massive hemorrhage in his left eye. Examination revealed an inferior wound dehiscence of approximately 8 clock hours (2 thru 10 o'clock) with prolapsed intraocular contents such as the uvea and retina. The patient underwent cornea graft resuturing with resection of ocular contents, which could not be repositioned. Although bleeding was controlled after the operation, vision was lost in his left eye. After two months, according to decrement of intraocular hematoma, the patient had a phthisis bulbi with low intraocular pressure in his left eye.
CONCLUSIONS
Persistent low intraocular pressure due to wound leakage through the graft-host junction likely resulted in delayed onset of expulsive suprachoroidal hemorrhage. The risk of traumatic corneal graft rupture after penetrating keratoplasty is significant and is associated with a poor visual outcome and eyeball viability. Therefore, patients should be cautioned. In addition, the importance of eye examination after trauma should be emphasized.
MeSH Terms
Figure
-

Figure 1. One year after penetrating keratoplasty.
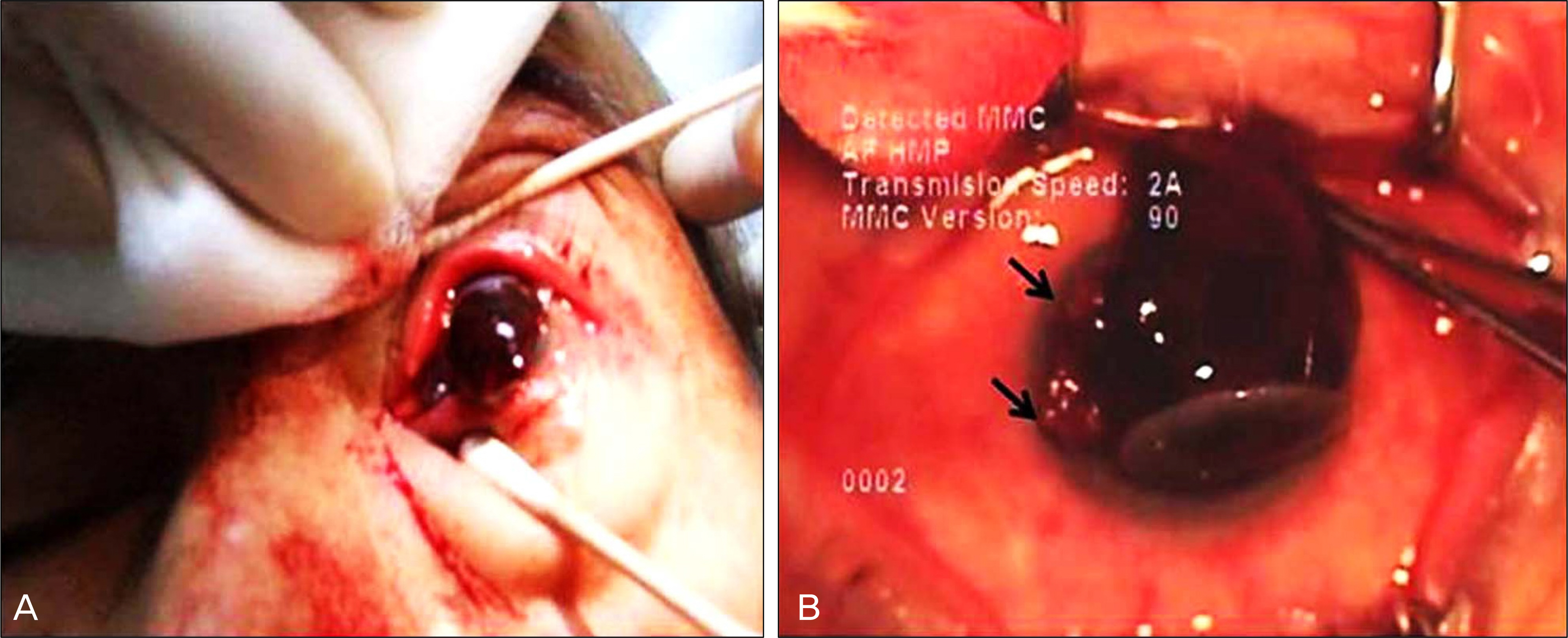
Figure 2. Two days after trauma. (A) Patient reveals massive hemorrhage with intraocular contents protruded through extensive corneal wound dehiscence. (B) Operator's view. Hinged corneal graft-host junction dehiscence is found from 2 to 10 o'clock site. Black arrows indicate protruding retinal and uveal tissues.
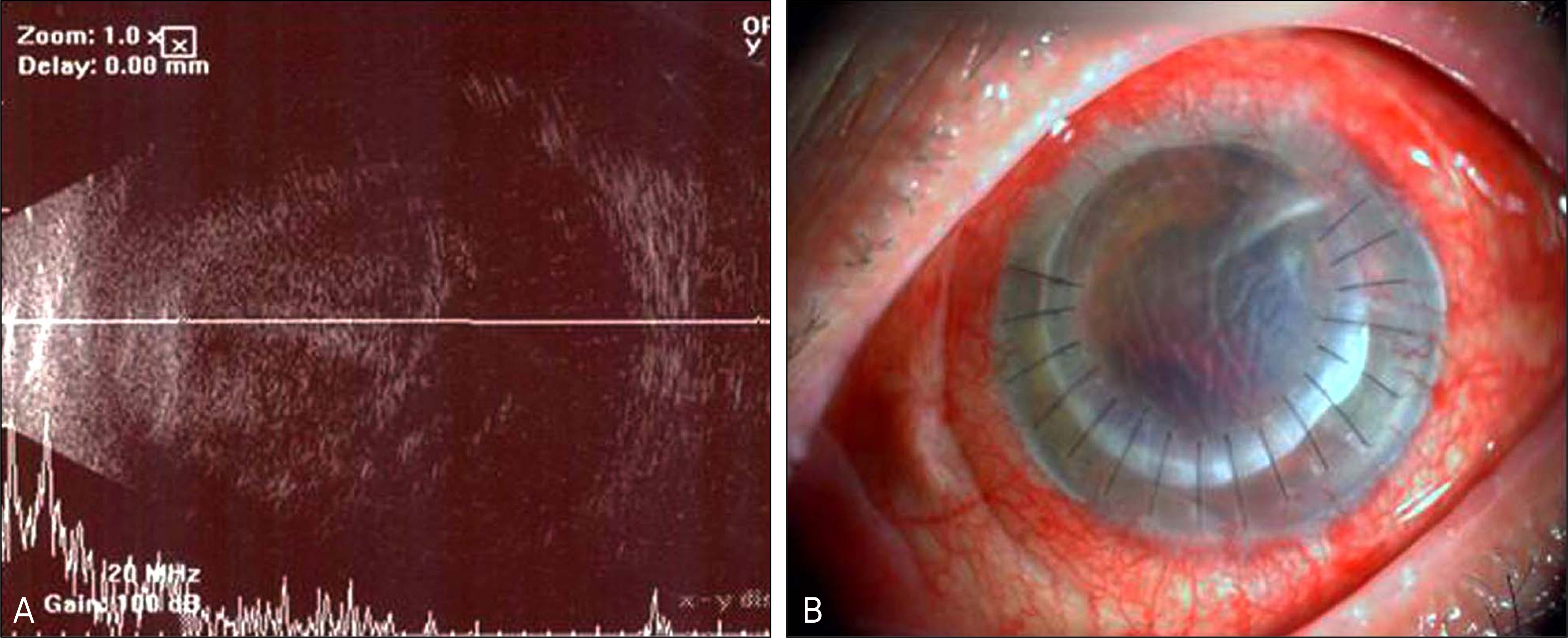
Figure 3. Ultrasound image and anterior segment photograph at postoperative one week.
Reference
-
References
1. Lee SJ, Cho EY, Kim MS. Clinical outcomes 10 years after penetrating keratoplasty. J Korean Ophthalmol Soc. 2006; 47:1043–8.2. Tseng SH, Lin SC, Chen FK. Traumatic wound dehiscence after penetrating keratoplasty: clinical features and outcome in 21 cases. Cornea. 1999; 18:553–8.3. Rehany U, Rumelt S. Ocular trauma following penetrating keratoplasty: incidence, outcome, and postoperative recommendations. Arch Ophthalmol. 1998; 116:1282–6.4. Elder MJ, Stack RR. Globe rupture following penetrating keratoplasty: how often, why, and what can we do to prevent it? Cornea. 2004; 23:776–80.5. Williams MA, Gawley SD, Jackson AJ, Frazer DG. Traumatic graft dehiscence after penetrating keratoplasty. Ophthalmology. 2008; 115:276–8.
Article6. Maheshwari S, Saswade M, Thool A. Traumatic wound dehiscence 14 years following penetrating keratoplasty. Indian J Ophthalmol. 2003; 51:259–60.7. Tran TH, Ellies P, Azan F, et al. Traumatic globe rupture following penetrating keratoplasty. Graefes Arch Clin Exp Ophthalmol. 2005; 243:525–30.
Article8. Lam FC, Rahman MQ, Ramaesh K. Traumatic wound dehiscence after penetrating keratoplasty - a cause for concern. Eye. 2007; 21:1146–50.9. Renucci AM, Marangon FB, Culbertson WW. Wound dehiscence after penetrating keratoplasty: clinical characteristics of 51 cases treated at Bascom Palmer Eye Institute. Cornea. 2006; 25:524–9.
Article10. Kim KS, Myong YW. Traumatic wound dehiscence after penetrating keratoplasty. J Korean Ophthalmol Soc. 1999; 40:2438–42.11. Koh T, Jung JY, Shim HS, Kim HK. Delayed Suprachoroidal hemorrhage after Ahmed valve implantation for neovascular glaucoma. J Korean Ophthalmol Soc. 2009; 50:635–9.
Article12. Lim HW, Ko BW, Song YM, Lee BR. Suprachoroidal hemorrhage during pars plana vitrectomy associated with valsalva maneuver. J Korean Ophthalmol Soc. 2008; 49:1022–7.
Article13. Nissman SA, Pasternak JF. Delayed-onset expulsive choroidal hemorrhage attributed to an acute elevation in systemic blood pressure following traumatic globe rupture. Ophthalmic Surg Lasers Imaging. 2005; 36:340–2.
Article14. Hiratsuka Y, Sasaki S, Nakatani S, Murakami A. Traumatic wound dehiscence after penetrating keratoplasty. Jpn J Ophthalmol. 2007; 51:146–7.
Article15. Meier P, Wiedemann P. Massive suprachoroidal hemorrhage: secondary treatment and outcome. Graefes Arch Clin Exp Ophthalmol. 2000; 238:28–32.
Article16. Wirostko WJ, Han DP, Mieler WF, et al. Suprachoroidal hemorrhage: outcome of surgical management according to hemorrhage severity. Ophthalmology. 1998; 105:2271–5.17. Pettinelli DJ, Starr CE, Stark WJ. Late traumatic corneal wound dehiscence after penetrating keratoplasty. Arch Ophthalmol. 2005; 123:853–6.
Article18. Abou-Jaoude ES, Brooks M, Katz DG, Van Meter WS. Spontaneous wound dehiscence after removal of single continuous penetrating keratoplasty suture. Ophthalmology. 2002; 109:1291–6.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Resolved Massive Suprachoroidal Hemorrhage after Sclerotomy in Penetrating Keratoplasty Patient
- Astigmatism after Penetrating Keratoplasty According to Suture Methods
- Changes in Astigmatism after Suture Removal in Penetrating Keratoplasty
- Changes in Corneal Curvature after Suture Removal in Penetrating Keratoplasty
- Suture Tension Adjustment of Single Running Suture in Penetrating Keratoplasty
