A Case of Needleless Jet Injector Induced Bilateral Chorioretinal Injury
- Affiliations
-
- 1Department of Ophthalmology, Myongji Hospital, College of Medicine, Kwandong University, Goyang, Korea. kimdk89@empal.com
- 2Department of Ophthalmology, College of Medicine, Kyunghee University, Seoul, Korea.
- KMID: 2212556
- DOI: http://doi.org/10.3341/jkos.2009.50.8.1282
Abstract
- PURPOSE
To report a case of bilateral chorioretinal injury by needleless jet injector misuse. CASE SUMMARY: In a dermatology department, the patient was diagnosed as having total alopecia and was scheduled to be injected on her eyelash by needleless jet injector for treatment but inexpert doctor injected on the eyelid, not eyelash, by mistake. She then suddenly complained of blurred vision and a floater just after that procedure and was referred to the ophthalmology department. Bilateral vitreous hemorrhage and preretinal hemorrhage were seen during indirect ophthalmoscopic examination and bilateral prophylactic argon laser photocoagulation was done around the suspicious tear site. Then bilateral vitreous hemorrhage and preretinal hemorrhage were absorbed and we found a partial retinal rupture lesion and choroidal rupture lesion in the right eye and a retinal injury lesion in the lefteye. Therefore we observed the lesions of both eyes continuously without further treatment. Her clinical symptoms improved. CONCLUSIONS: Needleless jet injector has many advantages, especially less pain and injury than a normal needle injector and is usually used in clinic as preoperative local anesthesia and steroid injection in many medical fields. In this case, the needleless injector was accidentally misused inducing both direct and indirect choroidal rupture and retinal injury. In general, while a needleless jet injector is used in ophthalmology department, we have to use it with the greatest care.
MeSH Terms
Figure
-
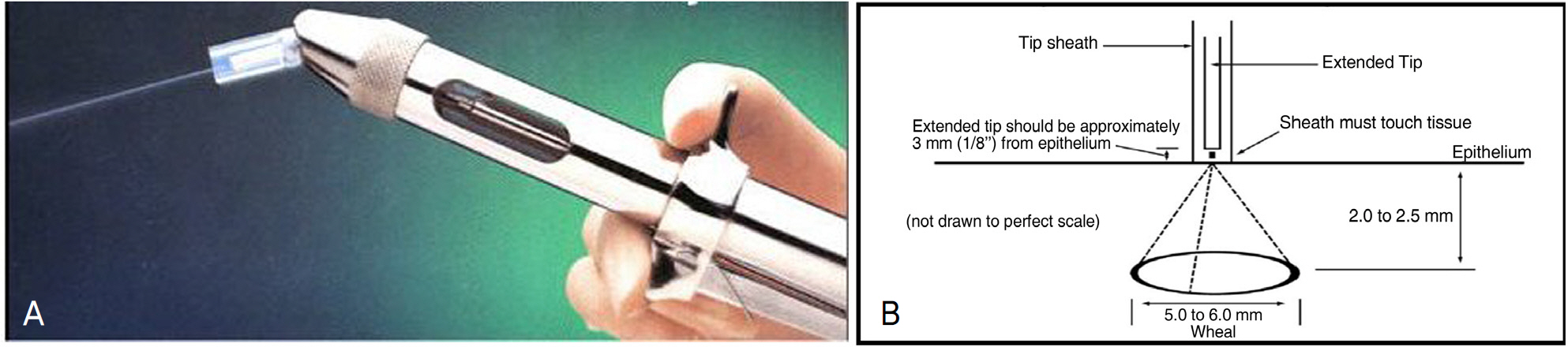
Figure 1. (A) Needless jet injector (B) Diagram illustrating device functions.

Figure 2. (A) Retinal injury and preretinal hemorrhage in superotemporal quadrant of left eye immediately after injury (before argon laser photocoagulation). (B) Choroidal rupture and preretinal hemorrhage covering lesions in superotemporal quadrant of right eye at two weeks after injury.
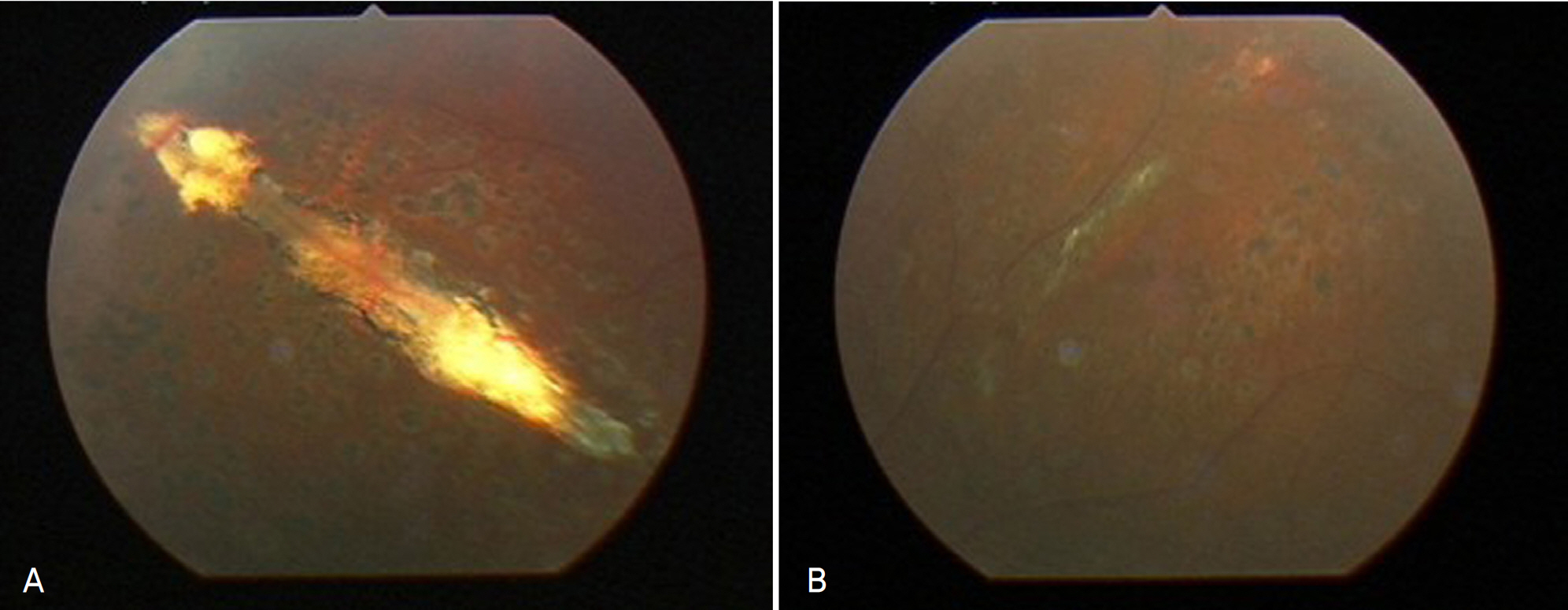
Figure 3. (A) Preretinal hemorrhage was absorbed clearly and full thickness and partial thickness choroidal rupture and retinal disruption were found in superotemporal quadrant of right eye at one year after injury. (B) Only the old laser scar was seen and old retinal injury was almost invisible in superotemporal quadrant of left eye at one year after injury.
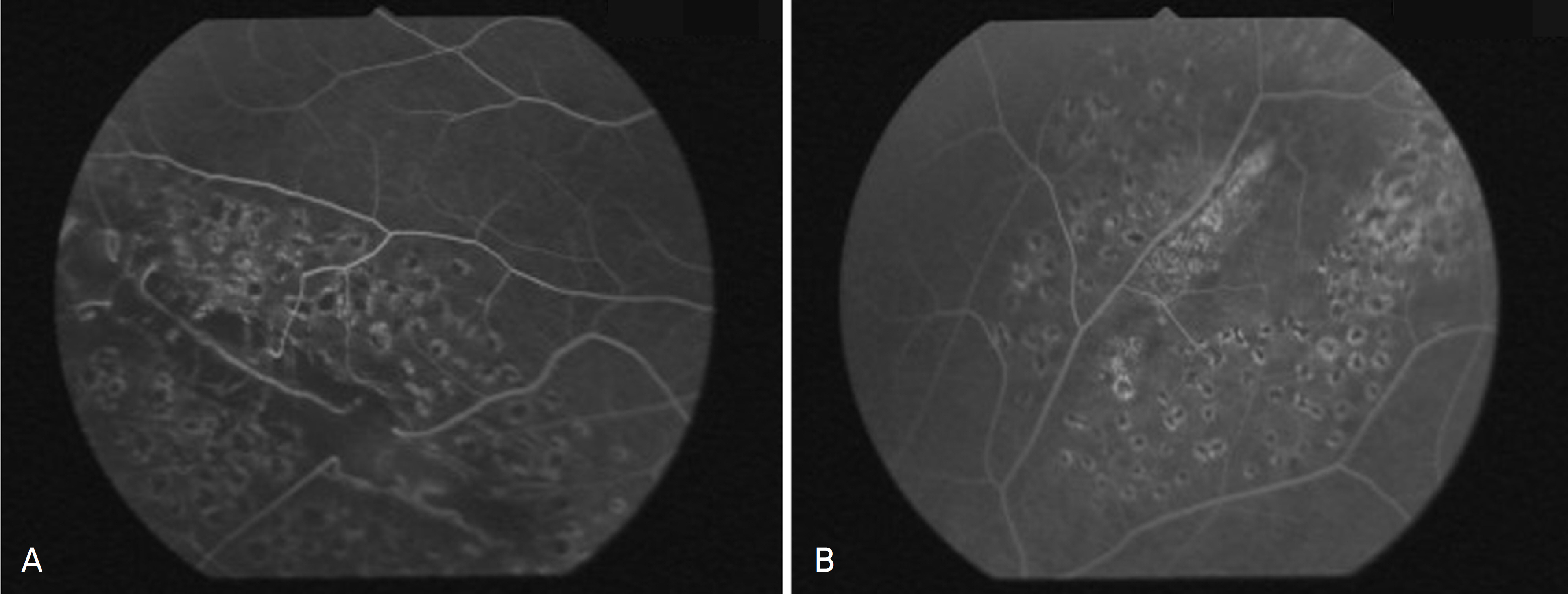
Figure 4. (A) Choroidal and retinal hypofluorescence at injury site in superotemporal area of right eye at 15 months after injury. (B) No remarkable finding but old laser scar was seen in superotemporal area of left eye at 15 months after injury.
Reference
-
References
1. Youssri AI, Young LH. Closed-globe contusion injuries of the posterior segment. Int Ophthalmol Clin. 2002; 42:79–86.
Article2. Dubinski W, Sharma S. Ophthalmoproblem. Can Fam Physician. 2006; 52:1071–9.3. Perry HT, Cohn BT, Nauheim JS. Accidental intraocular injection with Dermojet syringe. Arch Dermatol. 1977; 113:1131.
Article4. Wood CM, Richardson J. Indirect choroidal ruptures: aetiologic factors, patterns of ocular damage and final visual outcome. Br J Ophthalmol. 1990; 74:208–11.5. Eagling EM. Ocular damage after blunt trauma to the eye; its relationship to the nature of the injury. Br J Ophthalmol. 1974; 58:126–40.
Article6. Kaufer G, Zimmerman LE. Direct rupture of choroid. Arch Ophthalmol. 1966; 75:384–5.7. Duke-Elder WS. Textbook of Ophthalmology. 6. St. Louis: Mosby;1954. p. 5829–37.8. Aquilar JP, Green WR. Choroidal rupture A histopathologic study of 47 cases. Retina. 1984; 4:269–75.9. Benson WE, Shakin J, Sarin LK. Blunt trauma. Duane TD, Jaeger EA, editors. Clinical ophthalmology. Rev. ed.Philadelphia: Lippincott;1988. 3:chap. 1-7.10. Bressler SB, Bressler NM. Eye trauma. 1st ed.St Louis: Mosby Year Book;1991. p. 187–94.11. Wolter JR. Coup countercoup mechanism of ocular injuries. Am J Ophthalmol. 1963; 56:785–96.12. Delori F, Pomerantzeff O, Cox MS. Deformation of the globe under high speed impact: it relation to contusion injuries. Invest Ophthalmol Vis Sci. 1969; 8:290–301.13. Wiesenthal DT. Experimental ocular contusion. Arch Ophthalmol. 1964; 71:77–81.14. Gass JD. Stereoscopic atlas of macular diseases: diagnosis and treatment. 3rd ed.St Louis: Mosby;1987.15. Bisplinghoff JA, McNally C, Yang S, et al. High rate internal pre-ssurization of the human eye to determine ynamic rupture pressure. Biomed Sci Instrum. 2008; 44:117–22.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The feasibility of needleless jet injection versus conventional needle local anesthesia during dental procedures: a systematic review
- The Effect of Premedication using a Jet-injector in Pediatric Patients
- Airway Management of a Pediatric Patient with Interarytenoid Adhesion : A case report
- Vaginal injury from a high-pressure water jet in a prepubescent girl
- Combination treatment of a 1,064-nm picosecond domain Nd:YAG laser and a pneumatic needle-less injector for en coup de sabre in Republic of Korea: a case report
