J Korean Surg Soc.
2012 Oct;83(4):250-253. 10.4174/jkss.2012.83.4.250.
Endovascular treatment of ruptured infected aortic aneurysm with sepsis
- Affiliations
-
- 1Department of General Surgery, Daejeon St. Mary's Hospital, The Catholic University of Korea School of Medicine, Daejeon, Korea.
- 2Department of Thoracic and Cardiovascular Surgery, Daejeon St. Mary's Hospital, The Catholic University of Korea School of Medicine, Daejeon, Korea. phenix@catholic.ac.kr
- KMID: 2212320
- DOI: http://doi.org/10.4174/jkss.2012.83.4.250
Abstract
- The generally accepted treatment for infected aortic aneurysms involves open surgical resection and debridement, with in situ or extra-anatomical bypass. Occasionally, endovascular management can be substituted for the standard operation dependent on the patient's condition. We report the case of an 81-year-old female with a ruptured infected aortic aneurysm and sepsis, successfully treated endovascularly. She had been on oral antibiotics for one year and is doing well 2 years after discharge.
Keyword
MeSH Terms
Figure
-
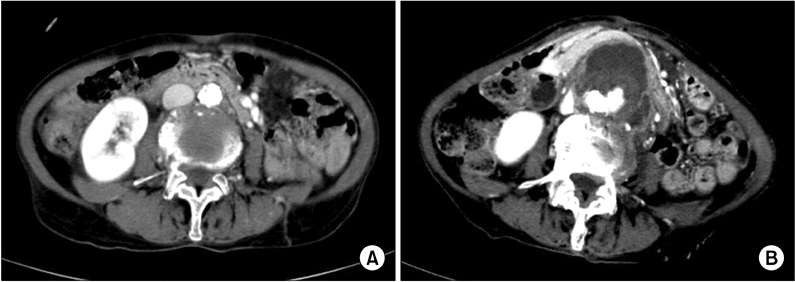
Fig. 1 (A) Contrast-enhanced computed tomography images revealed near normal abdominal aorta two months before admission and (B) ruptured abdominal aortic aneurysm at admission.

Fig. 2 (A) Endovascular treatment of right aorto-uni-iliac stent graft insertion, left common iliac artery plugging and fem-fem bypass and (B) follow-up computed tomography 3 months later angiogram revealed absorption of hematoma around the aorta.
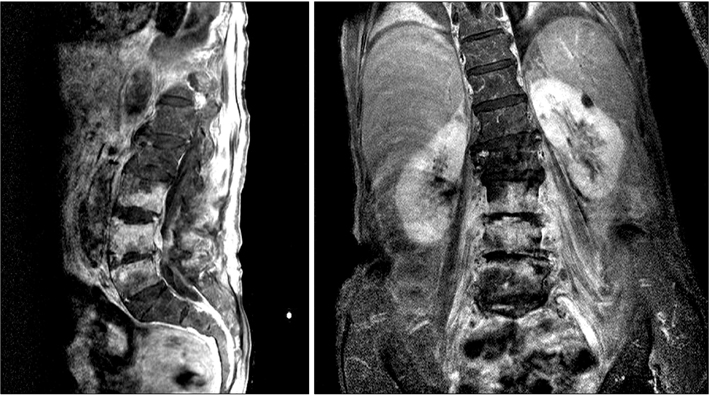
Fig. 3 Magnetic resonance imaging of the lumbosacral spine showed spondylitis in L3, 4, 5 levels, associated paraspinal and psoas muscle infection including microabscess.
Reference
-
1. Svensson LG, Crawford ES. Aortic dissection and aortic aneurysm surgery: clinical observations, experimental investigations, and statistical analyses. Part I. Curr Probl Surg. 1992. 29:817–911.2. Miller DV, Oderich GS, Aubry MC, Panneton JM, Edwards WD. Surgical pathology of infected aneurysms of the descending thoracic and abdominal aorta: clinicopathologic correlations in 29 cases (1976 to 1999). Hum Pathol. 2004. 35:1112–1120.3. Müller BT, Wegener OR, Grabitz K, Pillny M, Thomas L, Sandmann W. Mycotic aneurysms of the thoracic and abdominal aorta and iliac arteries: experience with anatomic and extra-anatomic repair in 33 cases. J Vasc Surg. 2001. 33:106–113.4. Hsu RB, Chen RJ, Wang SS, Chu SH. Infected aortic aneurysms: clinical outcome and risk factor analysis. J Vasc Surg. 2004. 40:30–35.5. Fillmore AJ, Valentine RJ. Surgical mortality in patients with infected aortic aneurysms. J Am Coll Surg. 2003. 196:435–441.6. Oderich GS, Panneton JM, Bower TC, Cherry KJ Jr, Rowland CM, Noel AA, et al. Infected aortic aneurysms: aggressive presentation, complicated early outcome, but durable results. J Vasc Surg. 2001. 34:900–908.7. Semba CP, Sakai T, Slonim SM, Razavi MK, Kee ST, Jorgensen MJ, et al. Mycotic aneurysms of the thoracic aorta: repair with use of endovascular stent-grafts. J Vasc Interv Radiol. 1998. 9(1 Pt 1):33–40.8. Kan CD, Lee HL, Yang YJ. Outcome after endovascular stent graft treatment for mycotic aortic aneurysm: a systematic review. J Vasc Surg. 2007. 46:906–912.9. Finlayson EV, Birkmeyer JD. Operative mortality with elective surgery in older adults. Eff Clin Pract. 2001. 4:172–177.10. Williamson WK, Nicoloff AD, Taylor LM Jr, Moneta GL, Landry GJ, Porter JM. Functional outcome after open repair of abdominal aortic aneurysm. J Vasc Surg. 2001. 33:913–920.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- General Considerations of Ruptured Abdominal Aortic Aneurysm: Ruptured Abdominal Aortic Aneurysm
- Ruptured Abdominal Aortic Aneurysm with Antecedent Endovascular Repair of Abdominal Aortic Aneurysm
- Abdominal Aortic Aneurysm
- Aortic Endograft Infection: Diagnosis and Management
- Successful Endovascular Treatment of an Infected Aortic Aneurysm Induced by Klebsiella pneumoniae
