J Korean Soc Spine Surg.
2006 Sep;13(3):200-204. 10.4184/jkss.2006.13.3.200.
Treatment of Upper Thoracic Disc Herniation Using Transthoracic Approach without Division of Latissimus Dorsi: Technical Note
- Affiliations
-
- 1Department of Orthopaedic Surgery, School of Medicine, Wonkwang University, Korea. llwind@hanmail.net
- 2Department of Orthopaedic Surgery, Gunsan Medical Center of Wonkwang University, Korea.
- 3Department of Orthopaedic Surgery, Kunpo Hospital of Wonkwang University, Korea.
- KMID: 2209642
- DOI: http://doi.org/10.4184/jkss.2006.13.3.200
Abstract
- Thoracic disc herniation is a rare condition in which a posterior approach, extrapleural approach, posterolateral approach, or transthoracic approach is currently used. The posterior approach is not recommended in thoracic disc herniation surgery because of the risk of spinal cord injury. The transthoracic approach makes it possible to remove the intervertebral disc and is considered a standard method. However, due to an extensive transverse skin incision, division of the latissimus dorsi muscles, and rib resection, the conventional open approaches involve a risk of complications, such as infection and post-thoracotomy pain syndrome; and a long period of rehabilitation and recovery is required. Excision of the intervertebral disc under thoracoscopic guidance can reduce the damage to the skin and muscles, but the equipment and surgical materials are expensive and a long learning curve is required. Therefore, we report a case and a new muscle splitting transthoracic approach that can be performed by incising 10 cm of skin longitudinally and preserving the serratus anterior and latissimus dorsi muscles.
MeSH Terms
Figure
-

Fig. 1. (A) Sagittal T2 weighted magnetic resonance image shows a disc extrusion at T3/4. (B) Axial T2 weighted magnetic resonance image shows a right posterolateral disc herniation.
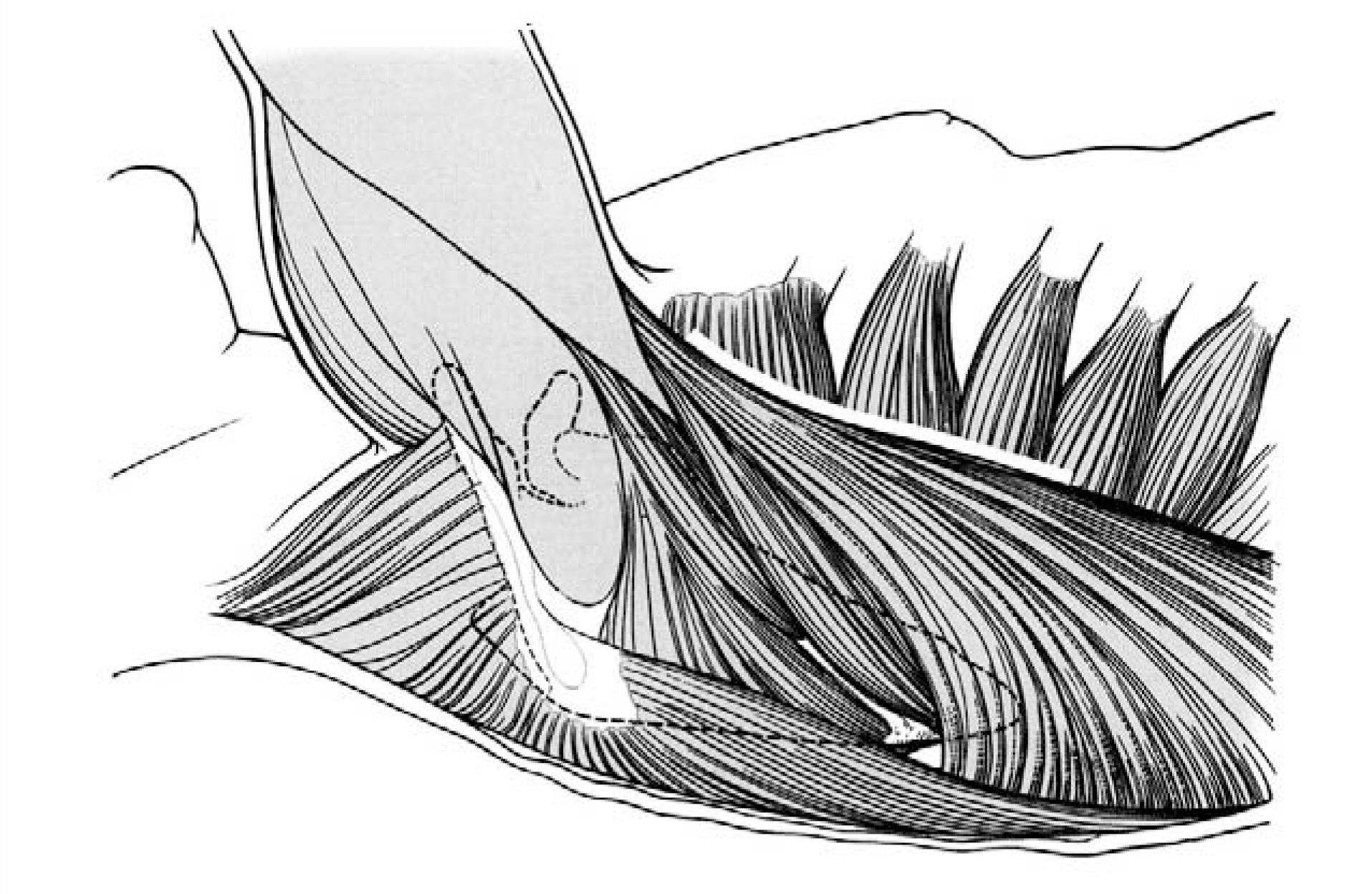
Fig. 2. White line indicates incision to be made in skin along the anterior border of latissimus dorsi muscle.
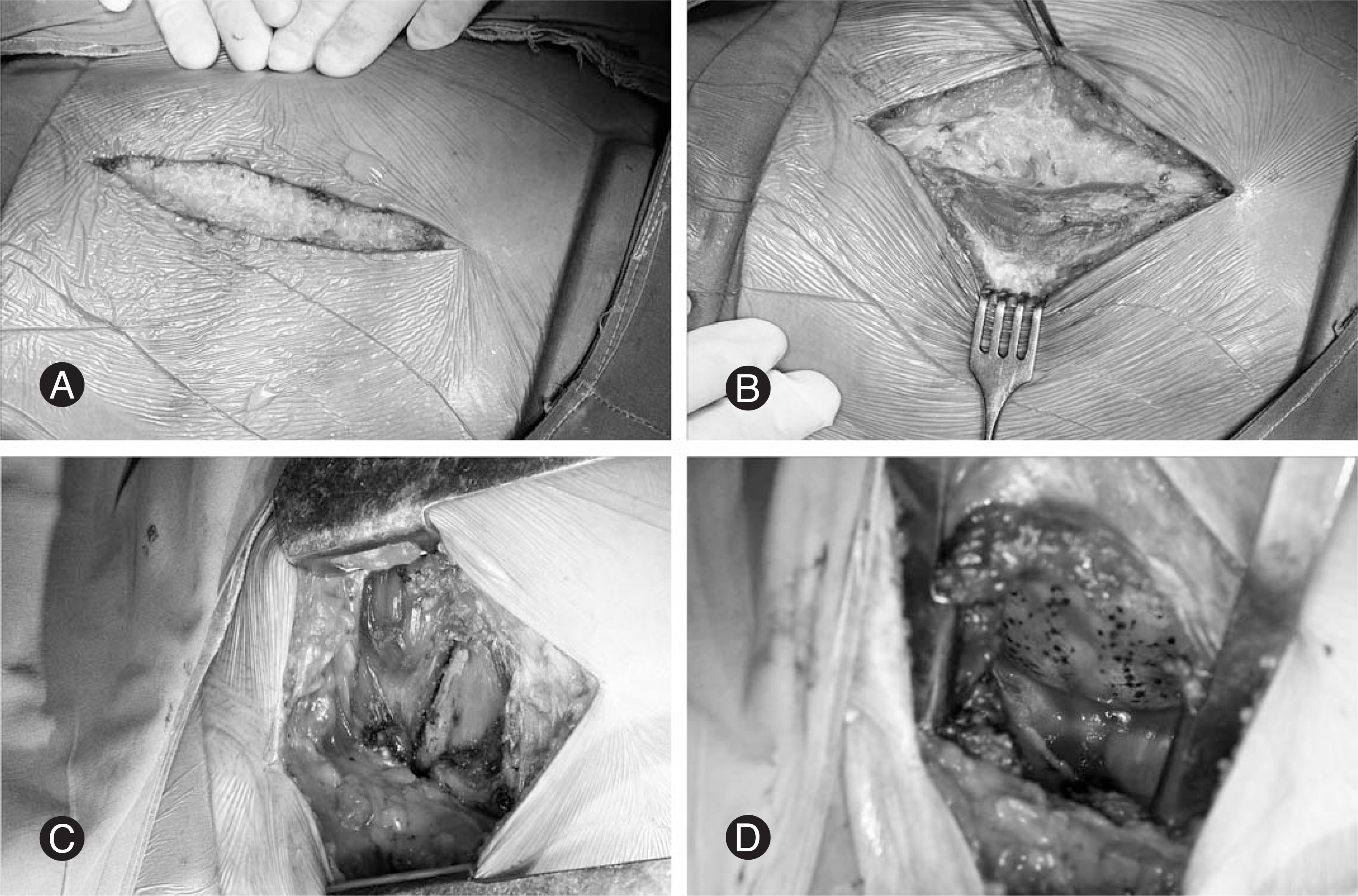
Fig. 3. (A) 10 cm straight longitudinal incision is made to skin along the anterior border of latissimus dorsi muscle. (B) Instead of dividing muscle, dissection is carried out between serratus anterior muscle and latissimus dorsi muscle to preserve them. (C) Latissimus dorsi muscle is retracted posteriorly by self retractor. (D) A rib spreader is inserted to hold the ribs apart.
Reference
-
01). Jefferson A. The treatment of thoracic intervertebral disc protrusions. Clin Neurol Neurosurg. 1975. 78:1–9.
Article02). Otani K., Yosida M., Fujii E., Nakai S., Shibasaki K. Thoracic disc herniation. Surgical treatment in 23patients. Spine. 1988. 13:1262–1267.03). Benson MK., Byrnes DP. The clinical syndromes and surgical treatment of thoracic intervertebral disc prolapse. J Bone Joint Surg Br. 1975. 57:471–477.
Article04). Patterson RH Jr., Arbit E. A surgical approach through the pedicle to protruded thoracic discs. J Neurosurg. 1978. 48:768–772.
Article05). Simpson JM., Silveri CP., Simeone FA., Balderston RA., An HS. Thoracic disc herniation. Re-evaluation of the posterior approach using a modified costotransversecto-my. Spine. 1993. 18:1872–1877.06). Mulier S., Debois V. Thoracic disc herniation: Transthoracic, lateral, or posterolateral approach? A review. Surg Neurol. 1998. 49:599–608.07). Fessler RG., Sturgill M. Review: Complications of surgery for thoracic disc disease. Surg Neurol. 1998. 49:609–618.
Article08). Regan JJ., Mack MJ., Picetti GD. A Technical report on video-assisted thoracoscopy in thoracic spinal surgery. Preliminary description. Spine. 1995. 20:831–837.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Thoracic Disc Herniation Treated by Transthoracic Transpleural Approach
- An Operative Case of Soft Disc Protrusion in Upper Thoracic Level: A Case Report
- Thoracic Disc Herniation Treated by Transthoracic Transpleural Approach
- Lateral Extracavitary Approach to Thoracic Cord Tumor and Disc Herniation
- Percutaneous Endoscopic Thoracic Discectomy in the Upper and Midthoracic Spine: A Technical Note
