Cystic Hypersecretory Carcinoma of the Breast: Sonographic Features with a Histological Correlation
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea. claudel@skku.edu
- 2Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Korea.
- KMID: 2208926
- DOI: http://doi.org/10.3348/jksr.2010.62.3.287
Abstract
- PURPOSE
To evaluate imaging findings of cystic hypersecretory carcinoma (CHC) of the breast, with an emphasis of the sonographic (US) features, and to correlate the US findings with the histology.
MATERIALS AND METHODS
During the last 13 years, six women with a mean age of 43 years were histologically confirmed with CHC of the breast. We retrospectively reviewed the clinical records, US images, and correlated them with histological findings.
RESULTS
US showed a large complex cystic mass lined by a thin wall (n = 2), multiple small cysts in focally heterogeneous background parenchyma without predominant mass (n = 3), and an irregular mass with an ill-defined margin and ductectasia (n = 1). The pathology revealed that the thin walls of the cysts were all cystic hypersecretory intraductal carcinomas, while the solid portions of the lesions varied from benign intraductal papillomas to minimal infiltrating ductal carcinoma in the background of the cystic hypersecretory intraductal carcinomas.
CONCLUSION
The characteristic US findings of cystic hypersecretory carcinoma are either a large complex cystic and solid mass or multiple small cysts in the background of a focally heterogeneous parenchyma.
MeSH Terms
Figure
-
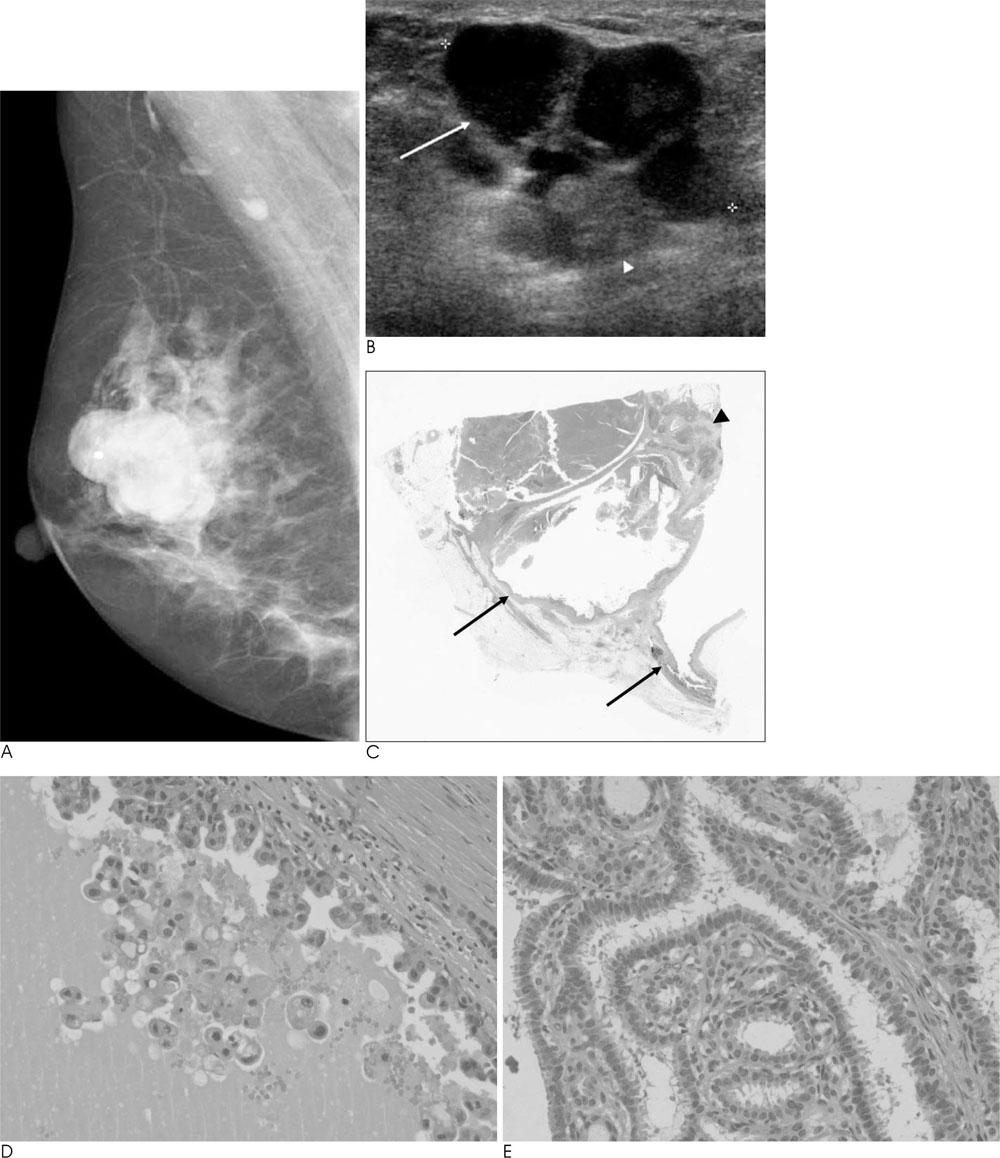
Fig. 1 A 52-year-old woman with cystic hypersecretory duct carcinoma of the right breast (Patient 6). A. Mediolateral oblique view of the mammography shows a hyperdense mass with lobulation, and without calcification in right upper outer breast. The mass shows relatively circumscribed, but a partially ill-defined margin in the posterior aspect. B. US shows a complex cystic (arrow) and solid (arrowhead) mass with a thin cystic wall. The solid portion is isoechoic and has an ill-defined margin. C. Histologically, the lesion consists of a few large cysts (arrow) and solid portions (arrowhead) (Hematoxylin-eosin stain, ×1). D, E. The cystic wall (D) and solid portion (E) of the tumor. Disorderly proliferation of the lining epithelium suggests evidence of cystic hypersecretory intraductal carcinoma in the cyst wall. Benign intraductal papilloma was seen in the solid portion (Hematoxylin-eosin stain, ×200).
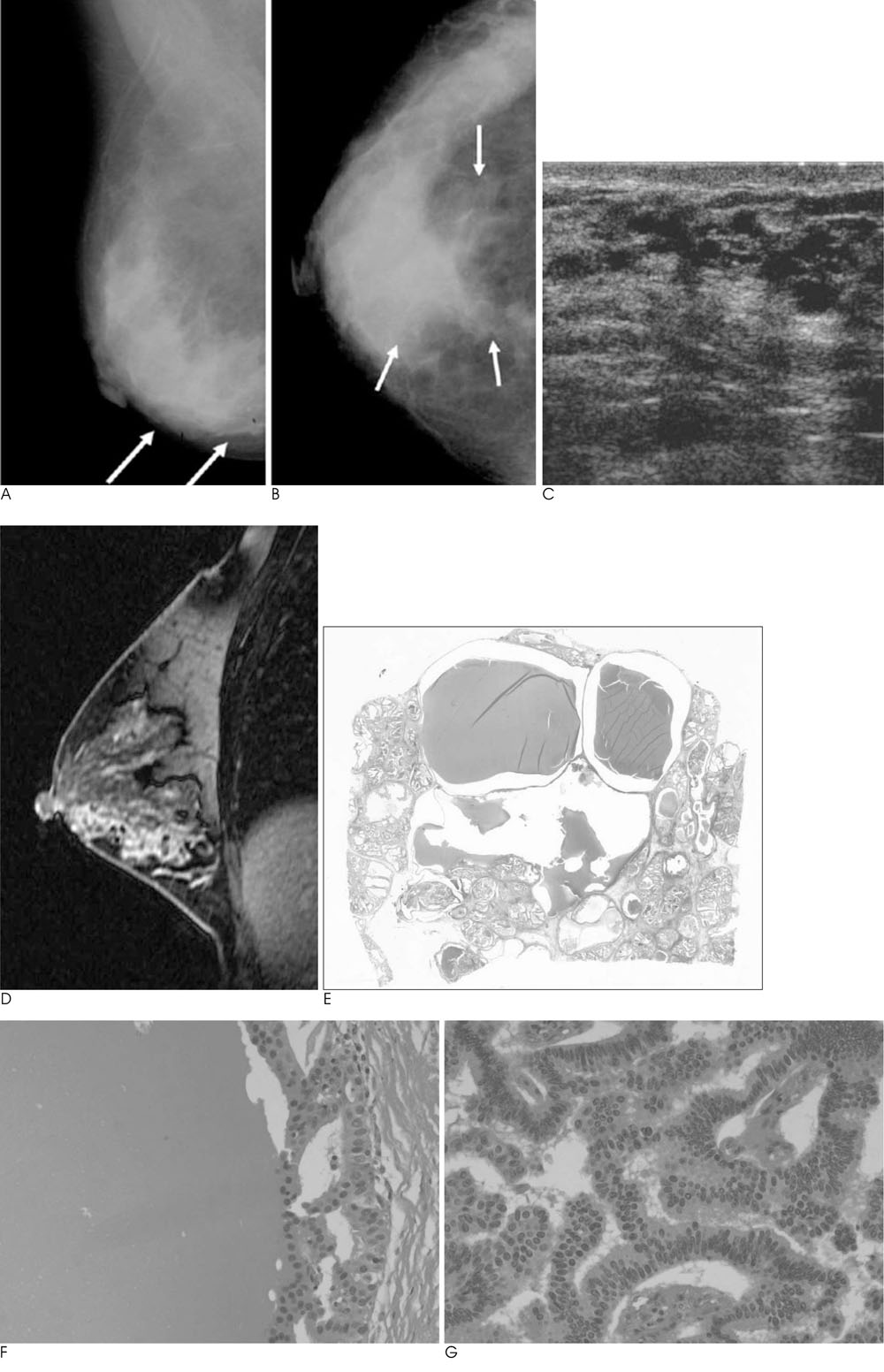
Fig. 2 A 46-year-old woman with cystic hypersecretory duct carcinoma of the right breast (Patient 4). A, B. Mediolateral oblique and craniocaudal views of the mammography show focal asymmetry with calcifications in right lower breast (arrows). C. US shows a complex cystic appearance and the solid lesion consists of multiple small irregular cysts in a focally heterogeneous background parenchyma without a predominant mass. D. A dynamic enhancement image of the lesion shows a segmental clumped nodular enhancement with multifocal small washout foci. E. Histologically, the lesion had numerous cysts containing secretions, ranging from 0.1 cm to 2 cm in diameter. The cysts expelled a hemorrhagic brownish and slightly mucoid fluid. Occasionally, some cysts contained more solid soft white-grayish tissue (Hematoxylin-eosin stain, ×1). F, G. Cystic wall (G) and solid portion (H) of the tumor. Both the wall of cysts and solid portion showed cystic hypersecretory intraductal carcinoma (Hematoxylin-eosin stain, ×200).
Reference
-
1. Rosen PP, Scott M. Cystic hypersecretory duct carcinoma of the breast. Am J Surg Pathol. 1984; 8:31–41.2. Guerry P, Erlandson RA, Rosen PP. Cystic hypersecretory hyperplasia and cystic hypersecretory duct carcinoma of the breast. Pathology, therapy, and follow-up of 39 patients. Cancer. 1988; 61:1611–1620.3. Herrmann ME, McClatchey KD, Siziopikou KP. Invasive cystic hypersecretory ductal carcinoma of breast: a case report and review of the literature. Arch Pathol Lab Med. 1999; 123:1108–1110.4. Kim MK, Kwon GY, Gong GY. Fine needle aspiration cytology of cystic hypersecretory carcinoma of the breast. A case report. Acta Cytol. 1997; 41:892–896.5. Lee WY, Cheng L, Chang TW. Diagnosing invasive cystic hypersecretory duct carcinoma of the breast with fine needle aspiration cytology. A case report. Acta Cytol. 1999; 43:273–276.6. Lee JS, Lee YJ. Invasive cystic hypersecretory carcinoma of the breast: a case report. J Korean Med Sci. 2004; 19:149–151.7. Shin SJ, Rosen PP. Carcinoma arising from preexisting pregnancy-like and cystic hypersecretory hyperplasia lesions of the breast: a clinicopathologic study of 9 patients. Am J Surg Pathol. 2004; 28:789–793.8. Park JM, Seo MR. Cystic hypersecretory duct carcinoma of the breast: report of two cases. Clin Radiol. 2002; 57:312–315.9. Park C, Jung JI, Lee AW, Cheon HM, Hahn ST, Lee JM. Sonographic findings in a patient with cystic hypersecretory duct carcinoma of the breast. J Clin Ultrasound. 2004; 32:29–32.10. Skalova A, Ryska A, Kajo K, Di Palma S, Kinkor Z, Michal M. Cystic hypersecretory carcinoma: rare and poorly recognized variant of intraductal carcinoma of the breast. Report of five cases. Histopathology. 2005; 46:43–49.11. Resetkova E, Padula A, Albarraccin CT, Sneige N. Pathologic quiz case: a large, ill-defined cystic breast mass. Invasive cystic hypersecretory duct carcinoma. Arch Pathol Lab Med. 2005; 129:e79–e80.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Invasive Cystic Hypersecretory Carcinoma of the Breast: A Case Report
- Intraductal Cystic Hypersecretory Carcinoma of the Breast: A case report
- Fine Needle Aspiration Cytology of Cystic Hypersecretory Intraductal Carcinoma of the Breast: Report of Two Cases
- Case of a Cystic Hypersecretory Duct Carcinoma of the Breast
- Clinical Mammographic, and Ultrasonographic Assessment of Breast Cancer Sizes
