CT Findings of Disease with Elevated Serum D-Dimer Levels in an Emergency Room Setting
- Affiliations
-
- 1Department of Radiology, Wonju Christian Hospital, Yonsei University Wonju College of Medicine, Wonju, Korea. wckwon@yonsei.ac.kr
- KMID: 2208877
- DOI: http://doi.org/10.3348/jksr.2012.66.1.93
Abstract
- Pulmonary embolism and deep vein thrombosis are the leading causes of elevated serum D-dimer levels in the emergency room. Although D-dimer is a useful screening test because of its high sensitivity and negative predictive value, it has a low specificity. In addition, D-dimer can be elevated in various diseases. Therefore, information on the various diseases with elevated D-dimer levels and their radiologic findings may allow for accurate diagnosis and proper management. Herein, we report the CT findings of various diseases with elevated D-dimer levels in an emergency room setting, including an intravascular contrast filling defect with associated findings in a venous thromboembolism, fracture with soft tissue swelling and hematoma formation in a trauma patient, enlargement with contrast enhancement in the infected organ of a patient, coronary artery stenosis with a perfusion defect of the myocardium in a patient with acute myocardial infarction, high density of acute thrombus in a cerebral vessel with a low density of affected brain parenchyma in an acute cerebral infarction, intimal flap with two separated lumens in a case of aortic dissection, organ involvement of malignancy in a cancer patient, and atrophy of a liver with a dilated portal vein and associated findings.
MeSH Terms
-
Atrophy
Brain
Cerebral Infarction
Coronary Stenosis
Emergencies
Fibrin Fibrinogen Degradation Products
Glycosaminoglycans
Hematoma
Humans
Liver
Mass Screening
Myocardial Infarction
Myocardium
Perfusion
Portal Vein
Pulmonary Embolism
Sensitivity and Specificity
Thrombosis
Venous Thromboembolism
Venous Thrombosis
Fibrin Fibrinogen Degradation Products
Glycosaminoglycans
Figure
-
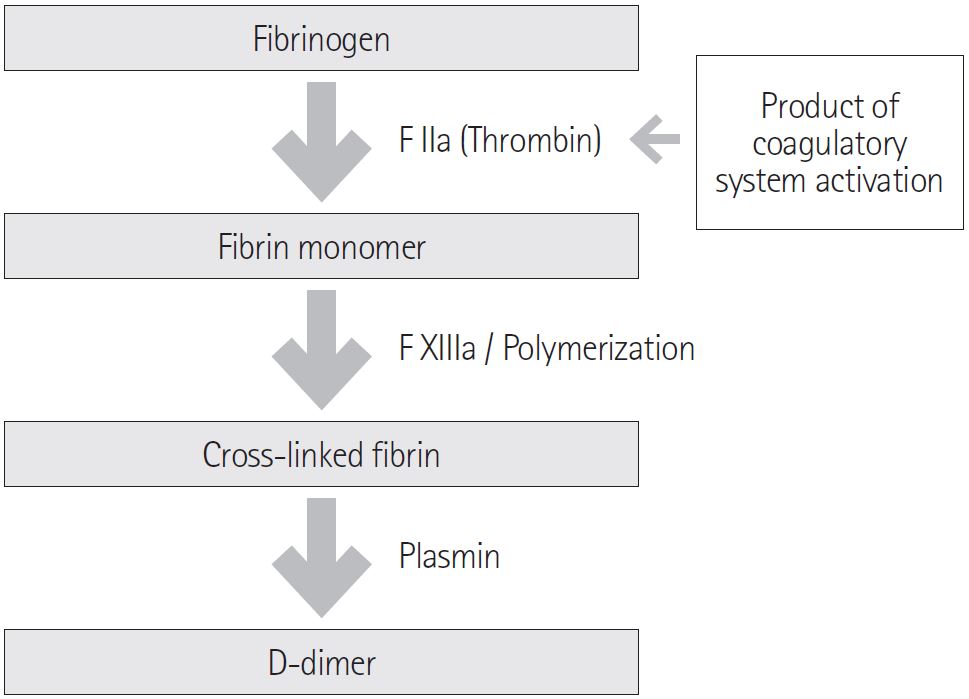
Fig. 1 Fibrin formation and fibrinolysis.

Fig. 2 A 27-year-old woman with an elevated serum D-dimer level (713 ng/mL). Axial CT lower extremity venography shows an intraluminal contrast filling defect within the dilated left femoral vein (arrow) and mild edematous change of the left lower extremity compared to the right side. The findings suggest acute deep vein thrombosis.

Fig. 3 An 18-year-old man with pulmonary embolism (serum D-dimer level: 19,653 ng/mL). Axial CT pulmonary angiography shows contrast filling defects within the bilateral pulmonary arteries (arrows).

Fig. 4 A 70-year-old man with burst fracture of the L2 vertebra (D-dimer level: 832 ng/mL). A. Lateral L-S spine shows the decreased height with biconcave shape of the L2 vertebral body (arrow). Note the fracture line of the lower endplate of the vertebra body. B. Axial CT L-spine shows the displaced bony fragment into the spinal canal (arrow) representing burst fracture.
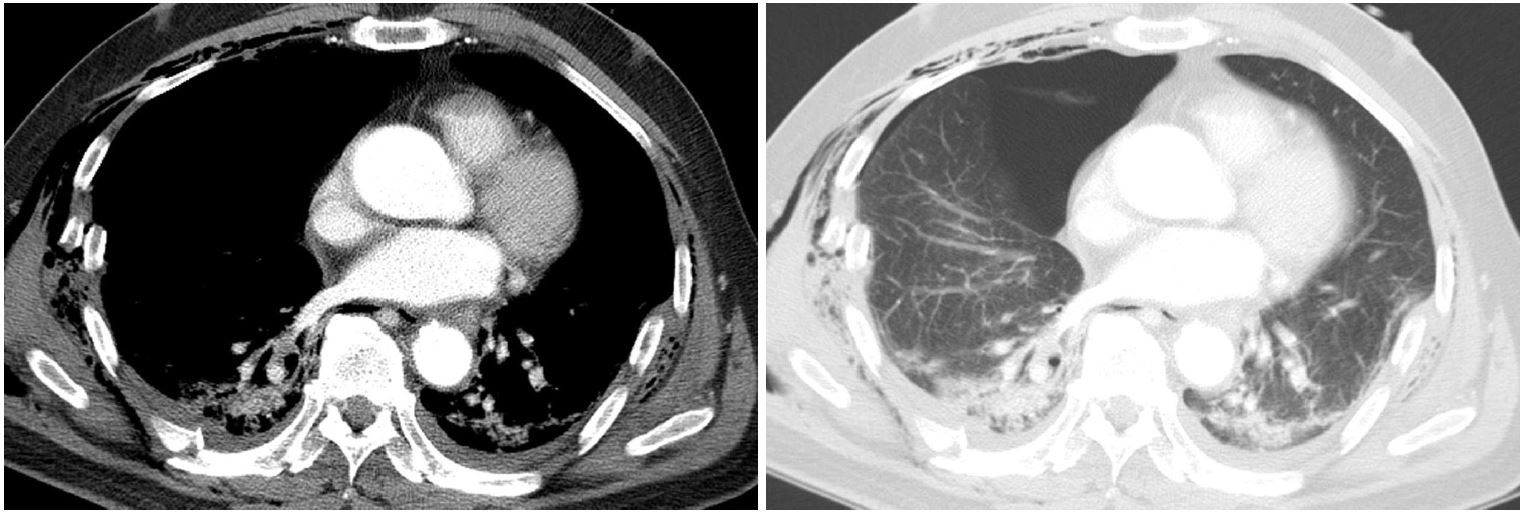
Fig. 5 A 73-year-old man with trauma (D-dimer level: 7,313 ng/mL). Axial CT chest scan shows bilateral multiple rib fractures with hemopneumothorax and subcutaneous emphysema suggesting traumatic thoracic injury.
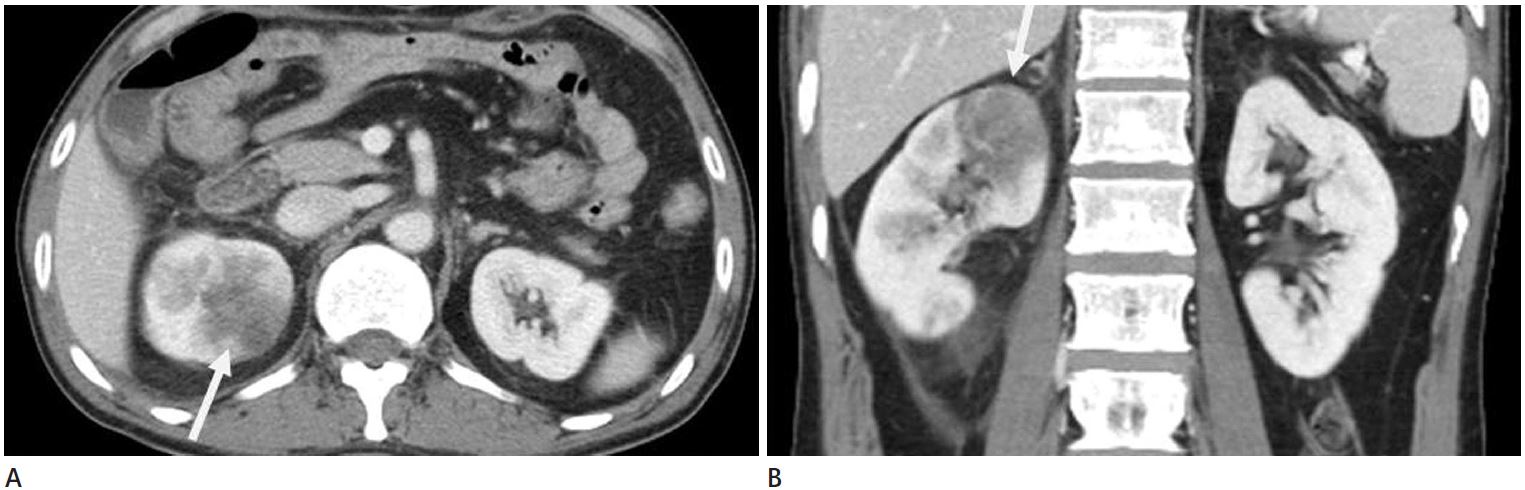
Fig. 6 A 48-year-old man with acute pyelonephritis (D-dimer: 932 ng/mL). Axial (A) and coronal (B) CT abdomen scans show a wedge shaped perfusion defect of the cortex of the right kidney (arrows), leading to loss of corticomedullary attenuation differentiation. Note the perinephric strand on the coronal scan indicating perinephric edematous change or inflammatory infiltration (B).

Fig. 7 A 79-year-old man with pneumonia and parapneumonic effusion (D-dimer level: 930 ng/mL). Axial CT pulmonary angiography shows consolidation in the right middle lobe and left lower lobe (B) with right pleural effusion (A). There was no pulmonary embolism.
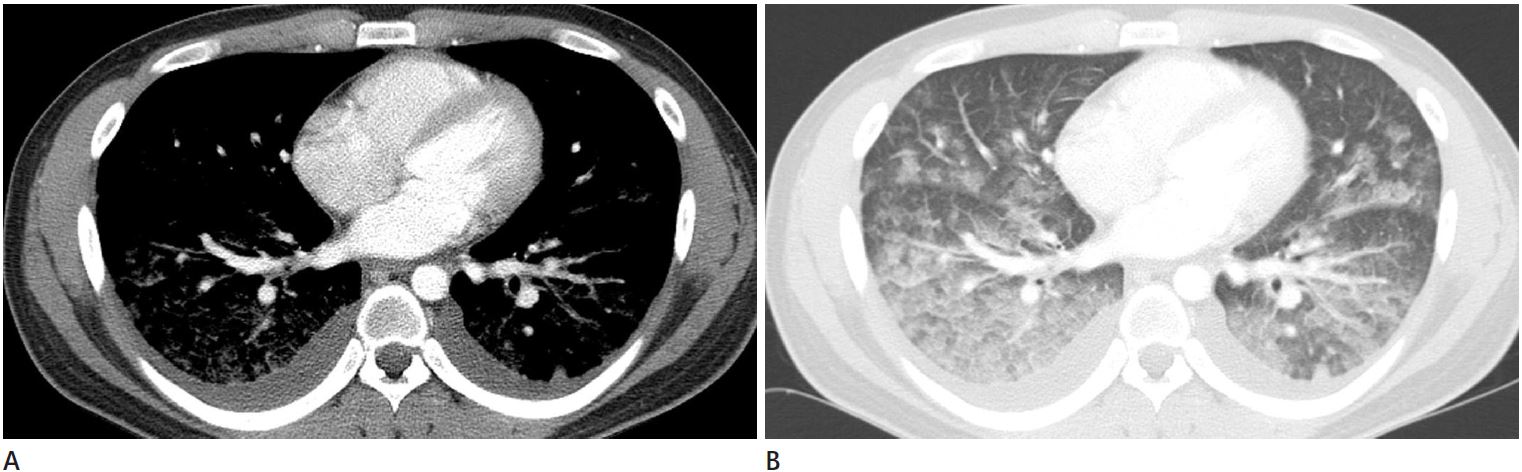
Fig. 8 A 22-year-old man with elevated serum D-dimer level (2,144 ng/mL). Axial CT chest scan shows bilateral diffuse ground glass opacities and consolidation in both lungs (B) with bilateral pleural effusion (A) representing acute eosinophilic pneumonia.

Fig. 9 A 48-year-old man with infectious enteritis (D-dimer level: 7,300 ng/mL). A. Axial CT abdomen scan shows a thickened wall of small bowel maintaining stratification (arrows). B. There are associated findings such as fluid collection in the right paracolic gutter (arrow) and several lymph nodes at the small bowel mesentery and paraaortic area.
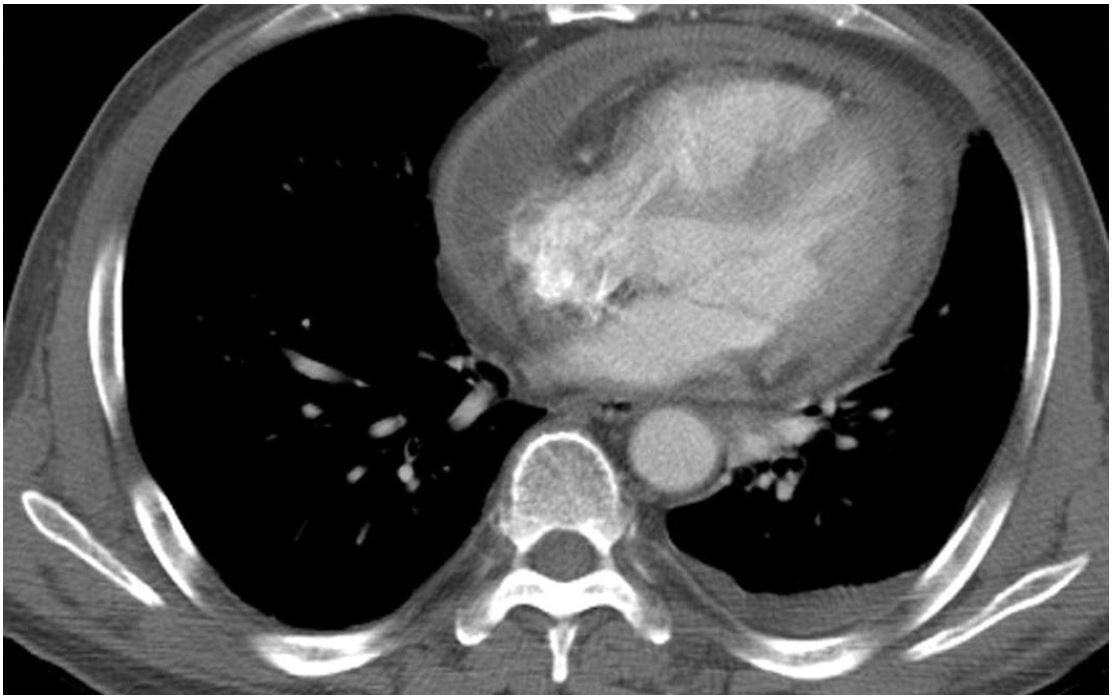
Fig. 10 A 67-year-old man with infectious pericarditis (D-dimer level: 2,003 ng/mL). Axial CT chest scan shows the thickened pericardium with contrast enhancement. Pericardial effusion was positive for tuberculosis real-time polymerase chain reaction. Left pleural effusion is also noted.
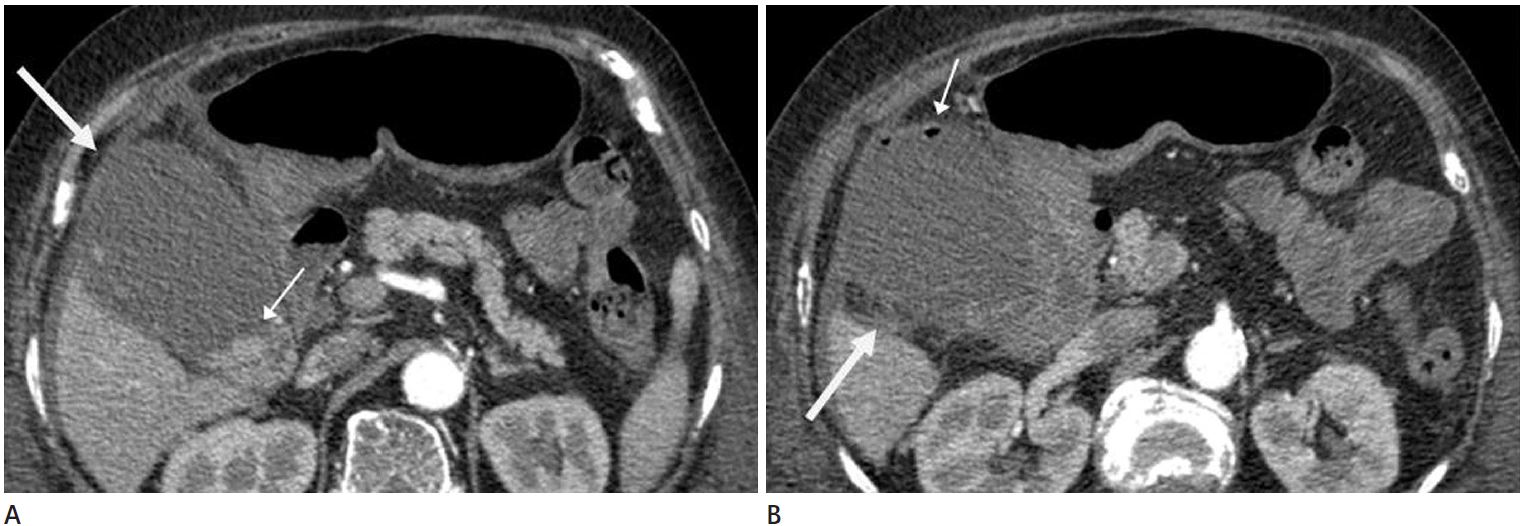
Fig. 11 A 81-year-old woman with gallbladder empyema (D-dimer level: 2,675 ng/mL). Axial CT pulmonary angiography shows a distended gall bladder (arrow), gallstones (small arrow) (A), intraluminal gas (small arrow), and adjacent fatty haziness (arrow) (B). Note enlarged lymph node along the common hepatic artery.

Fig. 12 A 40-year-old man with elevated serum D-dimer level (3,236 ng/mL). Axial CT abdomen scan shows an oval shaped poorly defined lesion at the left gluteus muscle with low density of the central portion and enhancing wall (arrow) suggesting intramuscular abscess. There are associated findings such as an enlarged left gluteus muscle and adjacent fatty strands.
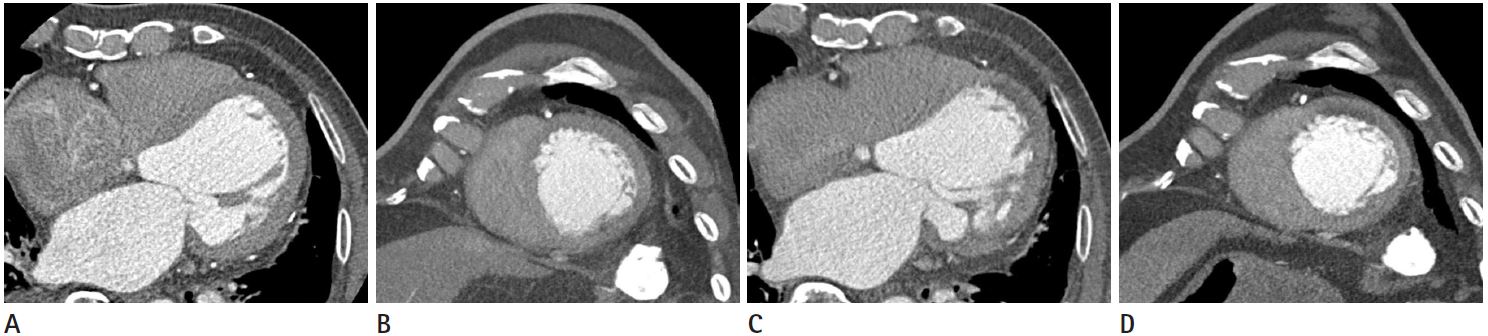
Fig. 13 A 84-year-old man with acute myocardial infarction (D-dimer level: 344 ng/mL). Axial (A) and short-axis (B) images of cardiac CT performed one year prior to the patient's current presentation show normal myocardial enhancement. Axial (C) and short-axis (D) images of cardiac CT performed during the period of acute symptom demonstrate hypoperfusion in the anterior wall of the left ventricle. The patient also had elevated serum cardiac enzymes and changed on electrocardiogram.
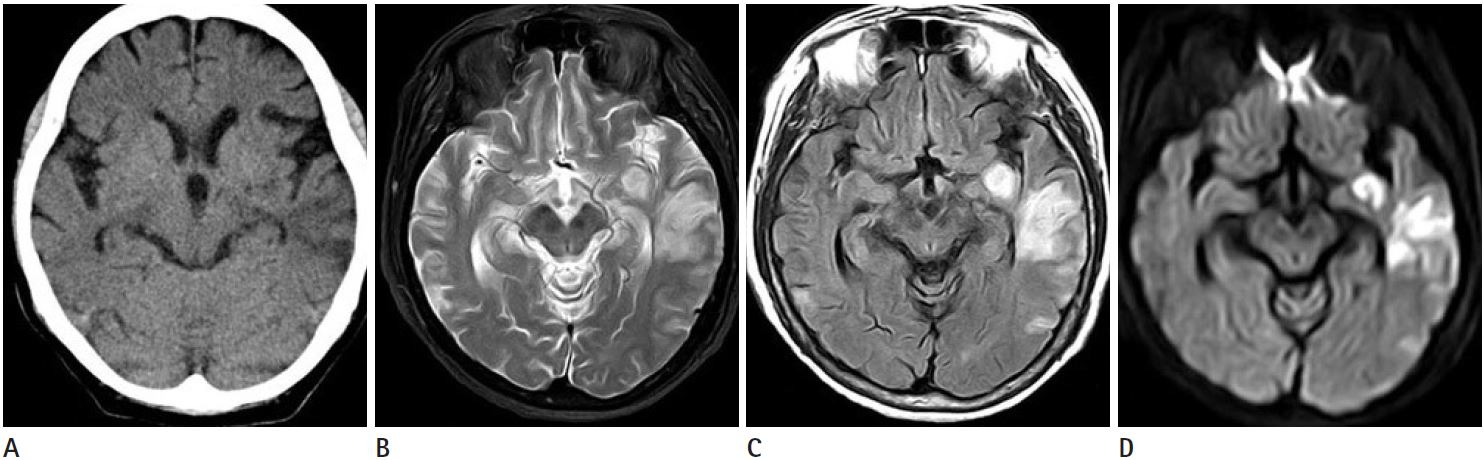
Fig. 14 A 65-year-old woman with recent cerebral infarction (D-dimer level: 1,949 ng/mL). Axial CT brain scan shows the ill defined low density lesion involving the gray and white matter of the left anterior temporal lobe with mild effacement of the left temporal cortical sulcal pattern (A). On MRI of the brain, the lesion shows high signal intensity on the axial T2-weighted image (B) and the fluid attenuated inversion recovery image (C), with diffusion restriction on the diffusion weighted image (D).
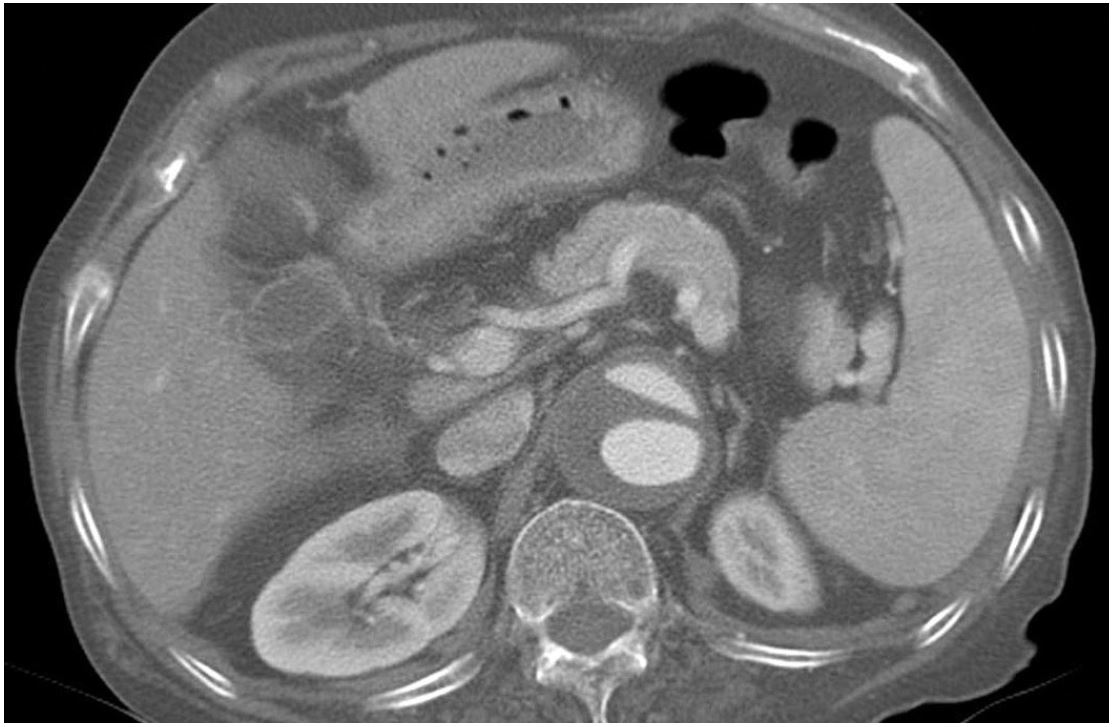
Fig. 15 A 69-year-old woman with elevated serum D-dimer level (1,238 ng/mL). Axial CT chest scan shows an intimal flap with two separated lumens in the dilated abdominal aorta suggesting aortic dissection.

Fig. 16 A 69-year-old man with lung cancer (D-dimer level: 869 ng/mL). Axial CT chest scan shows a lobular shaped mass with heterogeneous enhancement in the right upper lobe (final diagnosis, small cell carcinoma).

Fig. 17 A 50-year-old man with liver cirrhosis (D-dimer level: 3,914 ng/mL). Axial CT liver scan shows cirrhotic contour of liver with ascites and splenomegaly. A dilated splenic vein is also noted.
Reference
-
1. Lippi G, Franchini M, Targher G, Favaloro EJ. Help me, Doctor! My D-dimer is raised. Ann Med. 2008; 40:594–605.2. Park EA, Lee W, Lee MW, Choi SI, Jae HJ, Chung JW, et al. Chronic-stage deep vein thrombosis of the lower extremities: indirect CT venographic findings. J Comput Assist Tomogr. 2007; 31:649–656.3. Wittram C, Maher MM, Yoo AJ, Kalra MK, Shepard JA, McLoud TC. CT angiography of pulmonary embolism: diagnostic criteria and causes of misdiagnosis. Radiographics. 2004; 24:1219–1238.4. Shin YS, Kim YJ, Park IS, Chi HS. Alteration of coagulation and fibrinolysis in multiple trauma. J Korean Surg Soc. 1999; 57:172–179.5. Wang ZJ, Reddy GP, Gotway MB, Yeh BM, Hetts SW, Higgins CB. CT and MR imaging of pericardial disease. Radiographics. 2003; 23 Spec No:S167–S180.6. Beauchamp NJ Jr, Scott WW Jr, Gottlieb LM, Fishman EK. CT evaluation of soft tissue and muscle infection and inflammation: a systematic compartmental approach. Skeletal Radiol. 1995; 24:317–324.7. Arnett JH, Mohajer K, Okon SA. Evidence of acute myocardial infarction on CT. Br J Radiol. 2007; 80:e219–e221.8. Ohlmann P, Faure A, Morel O, Petit H, Kabbaj H, Meyer N, et al. Diagnostic and prognostic value of circulating D-Dimers in patients with acute aortic dissection. Crit Care Med. 2006; 34:1358–1364.9. Franchini M, Montagnana M, Targher G, Manzato F, Lippi G. Pathogenesis, clinical and laboratory aspects of thrombosis in cancer. J Thromb Thrombolysis. 2007; 24:29–38.10. Gram J, Duscha H, Zurborn KH, Bruhn HD. Increased levels of fibrinolysis reaction products (D-dimer) in patients with decompensated alcoholic liver cirrhosis. Scand J Gastroenterol. 1991; 26:1173–1178.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Course of Advanced Cancer Patients with Lower-Extremity Edema and Elevated D-dimer Levels who Underwent Computed Tomography Venography
- Correlation between plasma D-dimer levels and the severity of patients with chronic urticaria
- Differential diagnostic factors of type 1 and type 2 myocardial infarction in patients with elevated cardiac troponin levels
- Association between D-dimer and long-term mortality in patients with acute severe hypertension visiting the emergency department
- Serum D-dimer should not be used in the diagnosis of venous thromboembolism within 28 days of total knee replacement surgery
