Soft Tissue Masses Showing Low Signal Intensity on T2-weighted Images: Correlation with Pathologic Findings
- Affiliations
-
- 1Department of Radiology, Pusan National University Hospital, Busan, Korea. lis@pusan.ac.kr
- 2Department of Pathology, Pusan National University Hospital, Busan, Korea.
- 3Department of Radiology, Yeungnam University Hospital, Daegu, Korea.
- 4Department of Radiology, Keimyung University School of Medicine, Dongsan Medical Center, Daegu, Korea.
- 5Department of Radiology, Catholic Universiry of Daegu Hospital, Daegu, Korea.
- 6Department of Orthopedic Surgery, Pusan National University Hospital, Busan, Korea.
- KMID: 2206925
- DOI: http://doi.org/10.13104/jksmrm.2014.18.4.279
Abstract
OBJECTIVE
The aims of this article are to differentiate soft tissue masses showing low signal intensity on T2-weighted images (T2WIs) according to the histopathologic findings.
CONCLUSION
To know relatively small numbered soft tissue masses with low signal intensities on T2WIs adding characteristic location, morphology, signal intensities on other sequences might be helpful for differential diagnosis of mostly nonspecific soft tissue tumors on MRI.
Keyword
Figure
-

Fig. 1 61-year-old male patient with a fibroma of the tendon sheath. (a) On a coronal fat suppressed T2-weighted image, the mass located at the lateral aspect of the vastus lateralis muscle shows signal intensity equal to that of skeletal muscle. This finding is attributable to the high quantity of collagen in many of these tumors. (b) A photomicrograph (H & E staining, ×200) shows hypocellularity and the mass contains a dense collagenous matrix and scattered spindle-shaped fibroblasts.

Fig. 2 19-year-old male patient with nodular fasciitis. (a) On a sagittal fat-suppressed T2WI of the forearm, a well-defined soft tissue mass shows signal intensity higher than that of the subcutaneous fat and muscle. (b) A photomicrograph (H & E staining, ×400) shows increased cellularity. There are few foci of myxoid degeneration.

Fig. 3 40-year-old male patient with fibromatosis. (a) A mass located at the anterior chest wall shows signal intensity slightly higher than that of skeletal muscle on a T2WI. The mass contains a region with lower signal intensity. (b) A photomicrograph (H & E staining, ×100) shows a lesion that is predominantly fibrotic with low cellularity and with heavy collagen deposition.

Fig. 4 80-year-old male patient with a malignant fibrous histiocytoma. (a) On an axial T2WI of the right thigh, the mass located at the superficial aspect of the fascia shows intermediate signal intensity higher than that of skeletal muscle. (b) A photomicrograph (H & E staining, ×40) shows hypercellularity with a relatively low collagen content.

Fig. 5 64-year-old male patient with an elastofibroma. (a) An axial T2WI shows soft tissue with signal intensity similar to that of the adjacent skeletal muscle, interlaced with streaks of tissue with signal intensity of fat between the inferior margin of the scapula and posterior chest wall. This appearance corresponds to areas of dense fibrous connective tissue interlaced with areas of fat. (b) A photomicrograph (H & E staining, ×400) demonstrates scattered elastic fibers in a background of collagenous tissue. Relative hypocellularity is seen.

Fig. 6 45-year-old male patient with a fibrolipoma. (a) An axial T2WI shows the nonadipose component to have decreased signal intensity similar to that of muscle. Note the presence of adipose tissue in the interstices of the mass. (b) A photomicrograph (H & E staining, ×100) shows fibrolipomatous proliferation around the nerves (arrowheads). The presence of fibrous septae (arrow) is noted.

Fig. 7 31-year-old male patient with an amputation neuroma. (a) The mass (arrows) located at the ventral aspect of the distal portion of the amputated forearm shows a fascicular sign on an axial T2WI of the forearm. (b) A photomicrograph (H & E staining, ×100) shows numerous nerve bundles and the surrounding fibroblasts with a collagenous matrix.
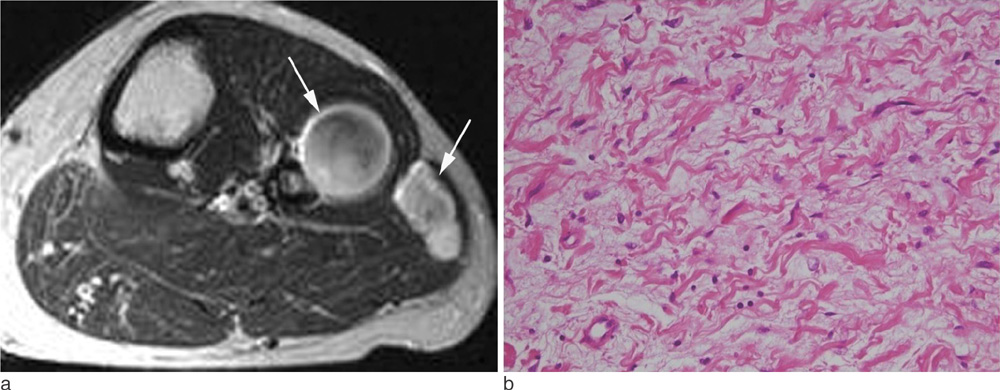
Fig. 8 34-year-old female patient with two neurofibromas. (a) An axial T2WI shows a well-defined mass with a center of low signal intensity and high signal intensity peripheral rim (target sign) through two muscular compartments. (b) A photomicrograph (H & E staining, ×200) shows scattered neurofibroma cells and a background of loosely packed collagen fibers and myxoid stroma.
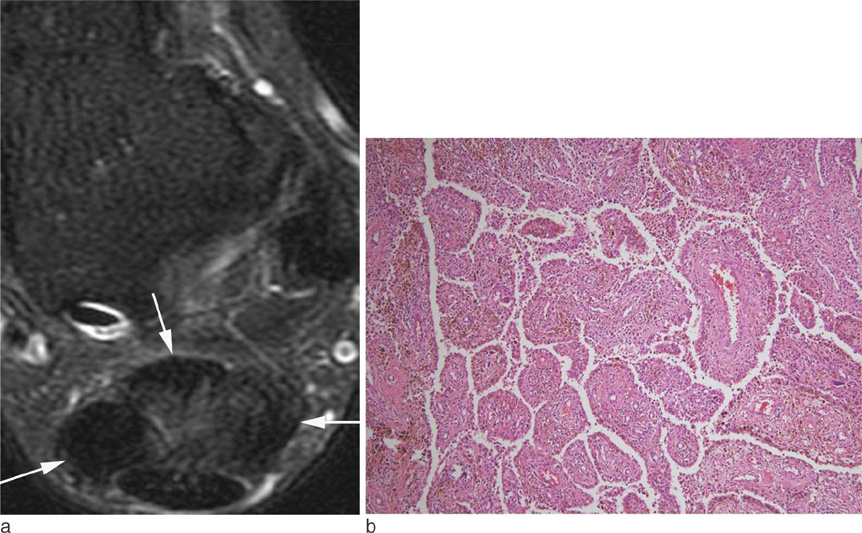
Fig. 9 33-year-old female patient with diffuse-type giant cell tumor(pigmented villonodular synovitis). (a) A fat-suppressed axial T2WI (a) shows a lobulated mass with low signal intensity in the retrocalcaneal bursa. (b) Photomicrographs (H & E staining, ×100) demonstrate the presence of multiple foci of hemosiderin deposits.

Fig. 10 60-year-old female patient with synovial osteochondromatosis. (a) On a sagittal T2WI of the ankle, multiple areas of signal void are noted within the effusion of the posterior ankle joint. (b) A corresponding plain radiograph shows the presence of multiple calcified nodules.

Fig. 11 40-year-old female patient with myositis ossificans. (a) A sagittal T2WI shows an inhomogeneous, well-defined mass surrounded by diffuse edema in the anteromedial aspect of the upper arm. The mass is surrounded by a thin hypointense rim, representing peripheral ossification. (b) As seen on a plain radiograph, a faintly mineralized mass is present.

Fig. 12 11-year-old male patient with a pilomatricoma. (a) On a coronal T2WI, a heterogeneous low signal intensity mass is seen in the subcutaneous fat layer of the cheek. (b) A photomicrograph (H & E staining, ×40) shows calcifications and ossification.
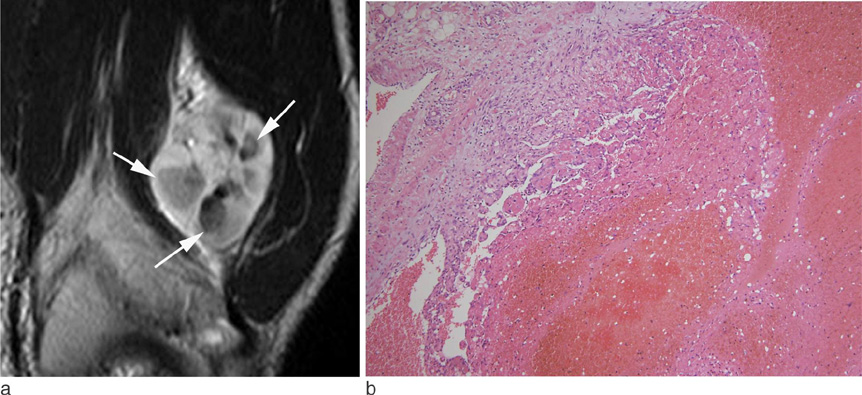
Fig. 13 25-year-old male patient with intravascular papillary endothelial hyperplasia. (a) A coronal T2WI of the thigh shows a well-defined mass with a hyperintense peripheral region and multiple hypointense or isointense central regions. (b) A photomicrograph (H & E staining, ×100) shows hemorrhage and a thrombus (arrows).

Fig. 14 26-year-old male patient with an alveolar soft part sarcoma. A coronal T2WI of the thigh shows a lobulated margined mass with higher signal intensity than that of the skeletal muscle and lower signal intensity than that of fat. Note the serpentine flow voids, representing enlarged blood vessels. Signal voids (arrows) are seen at the margin of the tumor.

Fig. 15 15-year-old male patient with an epidermoid cyst. (a) A coronal T2WI obtained through the abdominal wall shows a well-defined mass of intermediate to high signal intensity with dot-like low signal components in the subcutaneous fat layer. (b) A photomicrograph (H & E staining, ×100) shows keratin debris within the epithelial lining.
Cited by 1 articles
-
Focal Xanthogranulomatous Pyelonephritis Associated with Xanthogranulomatous Cholecystitis: A Case Report
Soong Moon Cho, Ho Kyun Kim, Hye Kyung Lee, Byungmo Lee, Ki Hwan Kim, Kyoung Eun Lee, Jae-Chan Shim, Dae Hyun Hwang, Ghi Jai Lee
J Korean Soc Radiol. 2020;81(1):190-196. doi: 10.3348/jksr.2020.81.1.190.
Reference
-
1. Sundaram M, McGuire MH, Schajowicz F. Soft-tissue masses: histologic basis for decreased signal (short T2) on T2-weighted MR images. AJR Am J Roentgenol. 1987; 148:1247–1250.2. Sundaram M, McLeod RA. MR imaging of tumor and tumorlike lesions of bone and soft tissue. AJR Am J Roentgenol. 1990; 155:817–824.3. Hur J, Damron TA, Vermont AI, Mathur SC. Fibroma of tendon sheath of the infrapatellar fat pad. Skeletal Radiol. 1999; 28:407–410.4. Fox MG, Kransdorf MJ, Bancroft LW, Peterson JJ, Flemming DJ. MR imaging of fibroma of the tendon sheath. AJR Am J Roentgenol. 2003; 180:1449–1453.5. Wang XL, De Schepper AM, Vanhoenacker F, et al. Nodular fasciitis: correlation of MRI findings and histopathology. Skeletal Radiol. 2002; 31:155–161.6. Blacksin MF, Ha DH, Hameed M, Aisner S. Superficial softtissue masses of the extremities. Radiographics. 2006; 26:1289–1304.7. Miettinen M, Fetsch JF. Collagenous fibroma (desmoplastic fibroblastoma): a clinicopathologic analysis of 63 cases of a distinctive soft tissue lesion with stellate-shaped fibroblasts. Hum Pathol. 1998; 29:676–682.8. Robbin MR, Murphey MD, Temple HT, Kransdorf MJ, Choi JJ. Imaging of musculoskeletal fibromatosis. Radiographics. 2001; 21:585–600.9. Dinauer PA, Brixey CJ, Moncur JT, Fanburg-Smith JC, Murphey MD. Pathologic and MR imaging features of benign fibrous soft-tissue tumors in adults. Radiographics. 2007; 27:173–187.10. Murphey MD, Gross TM, Rosenthal HG. From the archives of the AFIP. Musculoskeletal malignant fibrous histiocytoma: radiologic-pathologic correlation. Radiographics. 1994; 14:807–826. quiz 827-828.11. Mahajan H, Kim EE, Wallace S, Abello R, Benjamin R, Evans HL. Magnetic resonance imaging of malignant fibrous histiocytoma. Magn Reson Imaging. 1989; 7:283–288.12. Kransdorf MJ, Meis JM, Montgomery E. Elastofibroma: MR and CT appearance with radiologic-pathologic correlation. AJR Am J Roentgenol. 1992; 159:575–579.13. Murphey MD, Smith WS, Smith SE, Kransdorf MJ, Temple MT. From the archives of the AFIP. Imaging of musculoskeletal neurogenic tumors: radiologic-pathologic correlation. Radiographics. 1999; 19:1253–1280.14. Llauger J, Palmer J, Monill JM, Franquet T, Bagué S, Rosón N. MR imaging of benign soft-tissue masses of the foot and ankle. Radiographics. 1998; 18:1481–1498.15. Hassell DS, Bancroft LW, Kransdorf MJ, et al. Imaging appearance of diffuse neurofibroma. AJR Am J Roentgenol. 2008; 190:582–588.16. Llauger J, Palmer J, Roson N, Cremades R, Baque S. Pigmented villonodular synovitis and giant cell tumors of the tendon sheath: radiologic and pathologic features. AJR Am J Roentgenol. 1999; 172:1087–1091.17. Sheldon PJ, Forrester DM, Learch TJ. Imaging of intraarticular masses. Radiographics. 2005; 25:105–119.18. Murphey MD, Vidal JA, Fanburg-Smith JC, Gajewski DA. Imaging of synovial chondromatosis with radiologic-pathologic correlation. Radiographics. 2007; 27:1465–1488.19. Kransdorf MJ, Meis JM, Jelinek JS. Myositis ossificans: MR appearance with radiologic-pathologic correlation. AJR Am J Roentgenol. 1991; 157:1243–1248.20. Parikh J, Hyare H, Saifuddin A. The imaging features of posttraumatic myositis ossificans, with emphasis on MRI. Clin Radiol. 2002; 57:1058–1066.21. De Beuckeleer LH, De Schepper AM, Neetens I. Magnetic resonance imaging of pilomatricoma. Eur Radiol. 1996; 6:72–75.22. Lee SH, Suh JS, Lim BI, Yang WI, Shin KH. Intravascular papillary endothelial hyperplasia of the extremities: MR imaging findings with pathologic correlation. Eur Radiol. 2004; 14:822–826.23. Clifford PD, Temple HT, Jorda M, Marecos E. Intravascular papillary endothelial hyperplasia (Masson's tumor) presenting as a triceps mass. Skeletal Radiol. 2004; 33:421–425.24. Murphey MD, Fairbairn KJ, Parman LM, Baxter KG, Parsa MB, Smith WS. From the archives of the AFIP. Musculoskeletal angiomatous lesions: radiologic-pathologic correlation. Radiographics. 1995; 15:893–917.25. Vilanova JC, Barcelo J, Smirniotopoulos JG, et al. Hemangioma from head to toe: MR imaging with pathologic correlation. Radiographics. 2004; 24:367–385.26. Jones BC, Sundaram M, Kransdorf MJ. Synovial sarcoma: MR imaging findings in 34 patients. AJR Am J Roentgenol. 1993; 161:827–830.27. Nakanishi K, Araki N, Yoshikawa H, Hashimoto T, Nakamura H. Alveolar soft part sarcoma. Eur Radiol. 1998; 8:813–816.28. Hong SH, Chung HW, Choi JY, Koh YH, Choi JA, Kang HS. MRI findings of subcutaneous epidermal cysts: emphasis on the presence of rupture. AJR Am J Roentgenol. 2006; 186:961–966.29. Ruzek KA, Wenger DE. The multiple faces of lymphoma of the musculoskeletal system. Skeletal Radiol. 2004; 33:1–8.30. ter Braak BP, Guit GL, Bloem JL. Case 111: Soft-tissue lymphoma. Radiology. 2007; 243:293–296.31. Boukobza M, Mazel C, Touboul E. Primary vertebral and spinal epidural non-Hodgkin's lymphoma with spinal cord compression. Neuroradiology. 1996; 38:333–337.
