The Transmanubrial Approach for Cervicothoracic Junction Lesions : Feasibility, Limitations, and Advantages
- Affiliations
-
- 1Department of Neurosurgery, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon, Korea. isbrzw@gmail.com
- KMID: 2191372
- DOI: http://doi.org/10.3340/jkns.2015.58.3.236
Abstract
OBJECTIVE
We report on the technical feasibility and limitations of the transmanubrial approach for cervicothoracic junction (CTJ) lesions and emphasize the advantage of bisecting the upper part of the manubrium in an inverted Y-shape.
METHODS
Thirteen patients who underwent the fourteen transmanubrial approach for various CTJ lesions were enrolled during 2005-2014. For the evaluation of the accessibility for the CTJ lesion, we analyzed the two parallel line defined as a straight line parallel to the inferior and superior plateau of the upper and lower healthy vertebrae, the angle of the two parallel lines and the distance from the sternal notch to lines at the sternum on preoperative magnetic resonance images. Surgical limitations and perspectives, as well as postoperative clinical outcomes were evaluated retrospectively.
RESULTS
The CTJ lesions were six metastases, three primary bone tumors, two herniated discs, and one each of a traumatic dislocation with syrinx formation and tuberculous spondylitis and ossification of the posterior longitudinal ligament. If two parallel lines pass below the sternal notch, the manubriotomy should be inevitably performed. The mean preoperative Visual analogue scale score was 8 (range, 5-10), which improved to 4 (range, 0-6) postoperatively. Seven cases showed an increase in Frankel score postoperatively.
CONCLUSION
The spatial relationship between the sternal notch and the two parallel lines to the lesion was rational to determine the feasibility of manubriotomy. The transmanubrial approach for CTJ lesions can achieve favorable clinical outcomes by providing direct decompression of lesion and effective reconstruction.
MeSH Terms
Figure
-
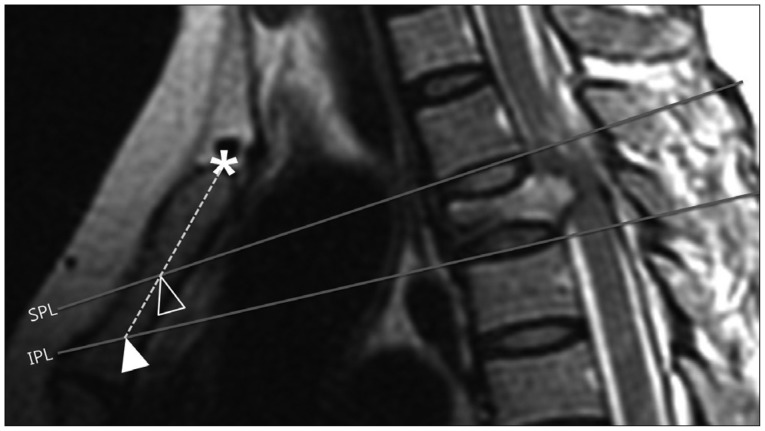
Fig. 1 The superior parallel line (SPL); a straight line parallel to the inferior plateau of the superior healthy vertebrae. The inferior parallel line (IPL); straight line parallel to the superior plateau of the inferior healthy vertebrae. The distances between the sternal notch to the SPL and IPL on the axis of the sternum were measured. * : sternal notch, empty arrow head : point of the SPL meets with sternum, filled arrow head : point of the IPL meets with the sternum.
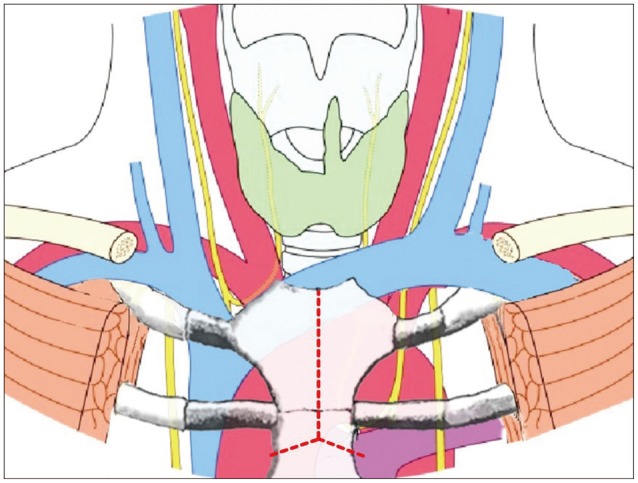
Fig. 2 Schematic illustration of anatomical structure around cervicothoracic junction and inverted Y-shape manubriotomy.
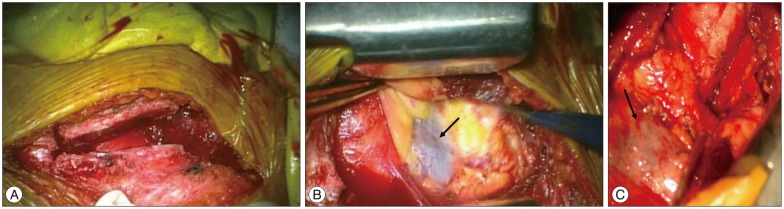
Fig. 3 Intraoperative photograph. A : bisecting manubrium as inverted Y-shaped with oscillating saw. B : Exposure of innominate vein (arrow) after bisecting manubrium after insertion of strong short retractor. C : Innominate vein (arrow) and other anterior visceral structures.
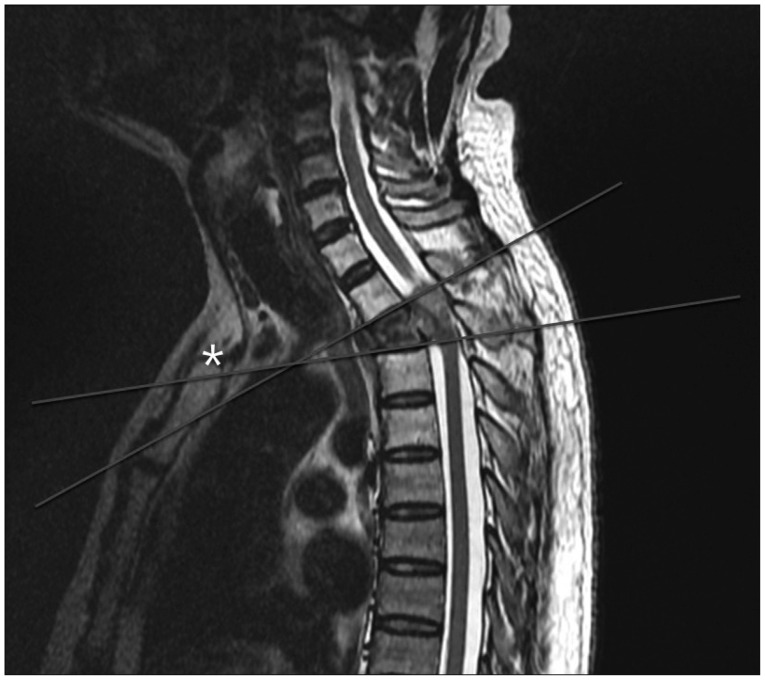
Fig. 4 57 years old man with T2 metastatic tumor. T2 weighted sagittal image shows tumor within T2 vertebral body distorting the cord.
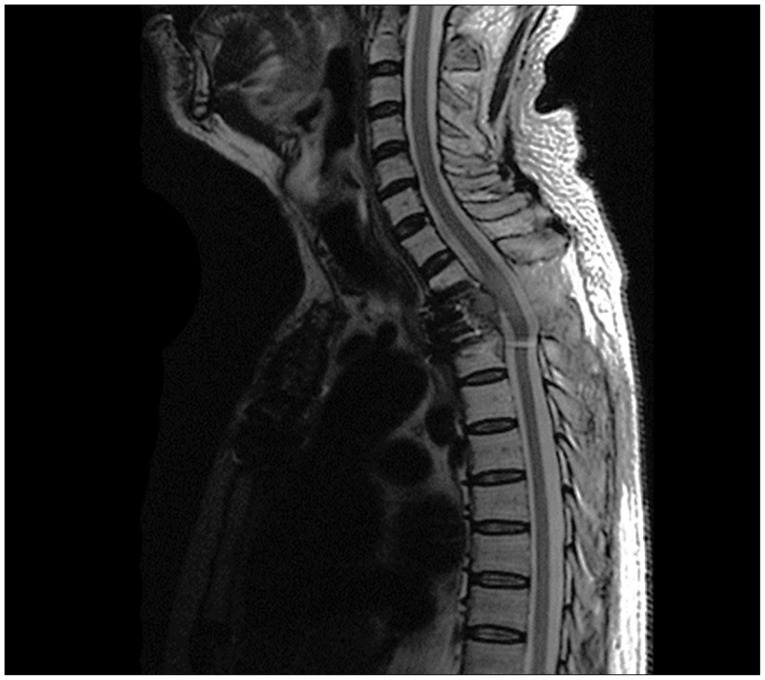
Fig. 5 Postoperative MR imaging shows corpectomy and reconstructed states at the T2 level.
Reference
-
1. Cauchoix J, Binet JP. Anterior surgical approaches to the spine. Ann R Coll Surg Engl. 1957; 21:237–243. PMID: 19310112.2. Cho W, Buchowski JM, Park Y, Maeda T, Nabb CE, Riew KD. Surgical approach to the cervicothoracic junction : can a standard Smith-Robinson approach be utilized. J Spinal Disord Tech. 2012; 25:264–267. PMID: 21566532.3. Cohen ZR, Fourney DR, Gokaslan ZL, Walsh GL, Rhines LD. Anterior stabilization of the upper thoracic spine via an "interaortocaval subinnominate window" : case report and description of operative technique. J Spinal Disord Tech. 2004; 17:543–548. PMID: 15570130.
Article4. Falavigna A, Righesso O, Teles AR. Anterior approach to the cervicothoracic junction : proposed indication for manubriotomy based on preoperative computed tomography findings. J Neurosurg Spine. 2011; 15:38–47. PMID: 21495813.
Article5. Fuentes S, Malikov S, Blondel B, Métellus P, Dufour H, Grisoli F. Cervicosternotomy as an anterior approach to the upper thoracic and cervicothoracic spinal junction. J Neurosurg Spine. 2010; 12:160–164. PMID: 20121350.
Article6. Huang YX, Ni WF, Wang S, Xu H, Wang XY, Xu HZ, et al. Anterior approaches to the cervicothoracic junction : a study on the surgical accessibility of three different corridors based on the CT images. Eur Spine J. 2010; 19:1936–1941. PMID: 20549258.
Article7. Huang YX, Tian NF, Chi YL, Wang S, Pan J, Xu HZ. Mini-open anterior approach to the cervicothoracic junction : a cadaveric study. Eur Spine J. 2013; 22:1533–1538. PMID: 23563573.
Article8. Karikari IO, Powers CJ, Isaacs RE. Simple method for determining the need for sternotomymanubriotomy with the anterior approach to the cervicothoracic junction. Neurosurgery. 2009; 65(6 Suppl):E165–E166. discussion E166PMID: 19935010.
Article9. Kaya RA, Türkmenoğlu ON, Koç ON, Genç HA, Cavuşoğlu H, Ziyal IM, et al. A perspective for the selection of surgical approaches in patients with upper thoracic and cervicothoracic junction instabilities. Surg Neurol. 2006; 65:454–463. discussion 463PMID: 16630904.
Article10. Kurz LT, Pursel SE, Herkowitz HN. Modified anterior approach to the cervicothoracic junction. Spine (Phila Pa 1976). 1991; 16(10 Suppl):S542–S547. PMID: 1801269.
Article11. Lapsiwala S, Benzel E. Surgical management of cervical myelopathy dealing with the cervical-thoracic junction. Spine J. 2006; 6(6 Suppl):268S–273S. PMID: 17097546.
Article12. Luk KD, Cheung KM, Leong JC. Anterior approach to the cervicothoracic junction by unilateral or bilateral manubriotomy. A report of five cases. J Bone Joint Surg Am. 2002; 84-A:1013–1017. PMID: 12063337.13. Pointillart V, Aurouer N, Gangnet N, Vital JM. Anterior approach to the cervicothoracic junction without sternotomy : a report of 37 cases. Spine (Phila Pa 1976). 2007; 32:2875–2879. PMID: 18246011.14. Sar C, Hamzaoglu A, Talu U, Domanic U. An anterior approach to the cervicothoracic junction of the spine (modified osteotomy of manubrium sterni and clavicle). J Spinal Disord. 1999; 12:102–106. PMID: 10229522.
Article15. Tarantino R, Donnarumma P, Marruzzo D, Landi A, De Giacomo T, Delfini R. Anterior surgical approaches to the cervicothoracic junction : when to use the manubriotomy? Spine J. 2013; 13:1064–1068. PMID: 23548505.
Article16. Teng H, Hsiang J, Wu C, Wang M, Wei H, Yang X, et al. Surgery in the cervicothoracic junction with an anterior low suprasternal approach alone or combined with manubriotomy and sternotomy : an approach selection method based on the cervicothoracic angle. J Neurosurg Spine. 2009; 10:531–542. PMID: 19558285.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Fractures and Dislocations of the Cervicothoracic Junction
- Cervicothoracic Junction Approach using Modified Anterior Approach: J-type Manubriotomy and Low Cervical Incision
- Inferiorly Migrated Disc Fragment at T1 Body Treated by T1 Transcorporeal Approach
- Supraclavicular Approach to a Lesion in the Cervico-Thoracic Junction
- Migrated Disc at Cervicothoracic Junction Presenting as Acute Paraplegia
