A New Measure for Monitoring Intraoperative Somatosensory Evoked Potentials
- Affiliations
-
- 1Department of Neurosurgery, Seoul National University Hospital, Seoul, Korea. chungc@snu.ac.kr
- 2Neuroscience Research Institute, Seoul National University Medical Research Center, Seoul, Korea.
- 3Department of Neurosurgery, Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Brain and Cognitive Sciences, Seoul National University College of Natural Sciences, Seoul, Korea.
- KMID: 2191129
- DOI: http://doi.org/10.3340/jkns.2014.56.6.455
Abstract
OBJECTIVE
To propose a new measure for effective monitoring of intraoperative somatosensory evoked potentials (SEP) and to validate the feasibility of this measure for evoked potentials (EP) and single trials with a retrospective data analysis study.
METHODS
The proposed new measure (hereafter, a slope-measure) was defined as the relative slope of the amplitude and latency at each EP peak compared to the baseline value, which is sensitive to the change in the amplitude and latency simultaneously. We used the slope-measure for EP and single trials and compared the significant change detection time with that of the conventional peak-to-peak method. When applied to single trials, each single trial signal was processed with optimal filters before using the slope-measure. In this retrospective data analysis, 7 patients who underwent cerebral aneurysm clipping surgery for unruptured aneurysm middle cerebral artery (MCA) bifurcation were included.
RESULTS
We found that this simple slope-measure has a detection time that is as early or earlier than that of the conventional method; furthermore, using the slope-measure in optimally filtered single trials provides warning signs earlier than that of the conventional method during MCA clipping surgery.
CONCLUSION
Our results have confirmed the feasibility of the slope-measure for intraoperative SEP monitoring. This is a novel study that provides a useful measure for either EP or single trials in intraoperative SEP monitoring.
Keyword
MeSH Terms
Figure
-
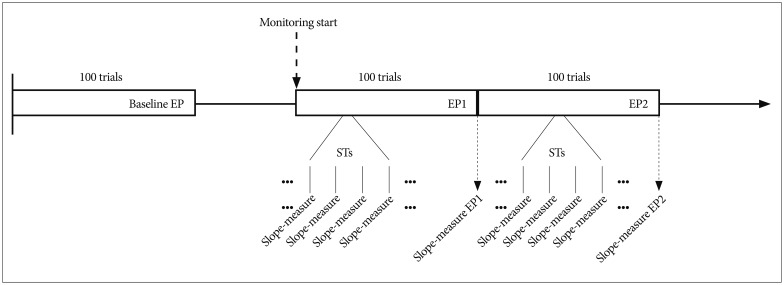
Fig. 1 Flow diagram of SEP detection and slope-measure application. Baseline value was determined before the main surgery, and when starting the surgery, the monitoring began. The slope-measure value of the EP was calculated after 100 trials, and the slope-measure values of the single trials (STs) were calculated for every single trial after applying a moving average filter. SEP : somatosensory evoked potentials, EP : evoked potentials.
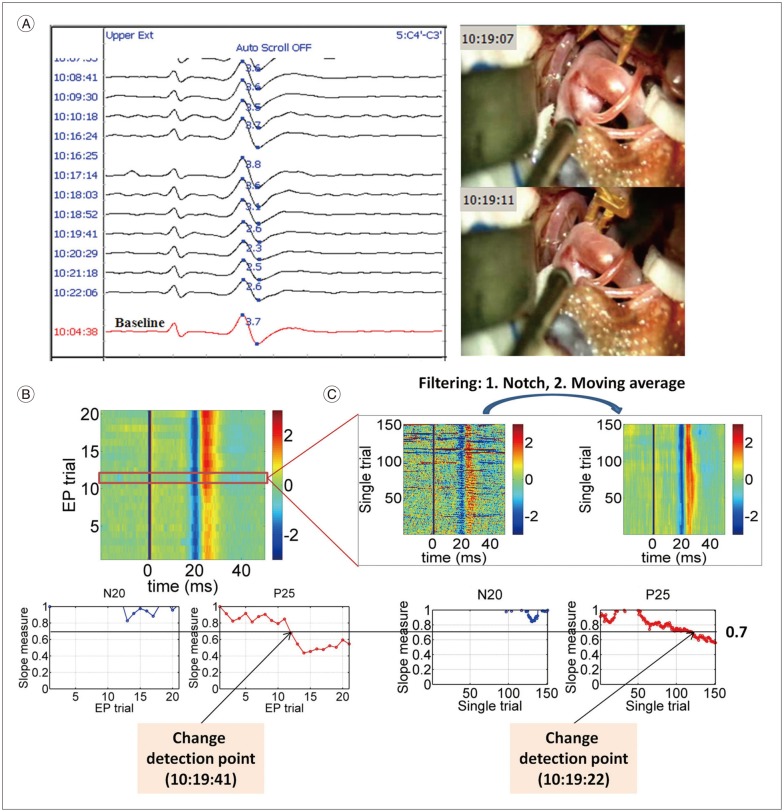
Fig. 2 Analysis process at the left upper extremity from Subject 1. A : The raw SEP monitoring data along with the video capture of the temporary clipping from Subject 1. Baseline (the red signal at the bottom) was determined at 10 : 04 : 38, and the peak-to-peak amplitude value at baseline was 3.7 (the blue figure on the baseline signal). The significant change with the conventional method was detected at 10 : 20 : 29 (2.3/3.7, i.e., 37.84% decrease to the baseline). A temporary clip was applied between the times 10 : 19 : 07 and 10 : 19 : 11. B : EP signals as a function of time (upper subpanel). In the upper subpanel, blue and red colors mean negative and positive voltage, respectively, and baseline signal corresponds to the first EP trial. In the lower subpanels, slope-measure values as a function of the EP trial of the N20 and P25 components were plotted. In this case, a significant change in the slope-measure of the EP was detected at 10 : 19 : 41 (45.45% decrease to the baseline). C : Single trials signals as a function of time (upper subpanel). The noise in the single trials was remarkably reduced by applying filters. In the lower subpanels, slope-measure values as a function of the single trial of the N20 and P25 components were plotted. In this case, a significant change in the slope-measure of the single trial was detected at 10 : 19 : 22 (37.59% decrease to the baseline). SEP : somatosensory evoked potentials, EP : evoked potentials.
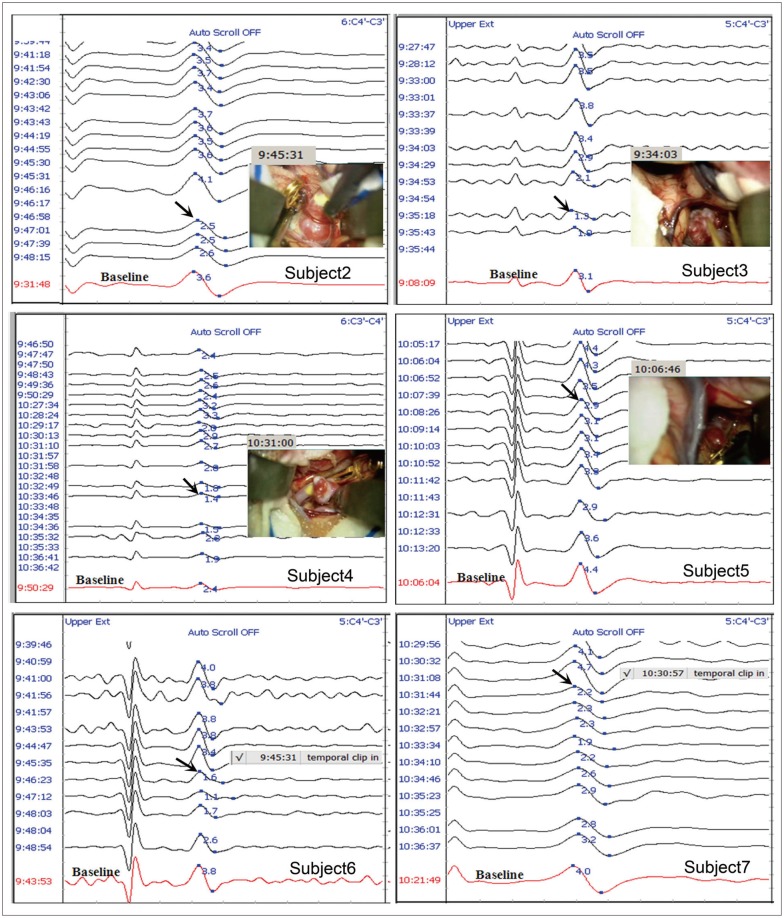
Fig. 3 Raw SEP data and video capture or comments showing the temporary clipping time at the contralateral upper extremity to the aneurysm from Subject 2 to Subject 7. The red signal at the bottom in each sub-graph corresponds to the baseline. The number in blue font on the baseline signal indicates the conventional peak-to-peak amplitude. The black arrow indicates a significant SEP change. SEP : somatosensory evoked potentials.
Reference
-
1. Bai O, Nakamura M, Nagamine T, Shibasaki H. Parametric modeling of somatosensory evoked potentials using discrete cosine transform. IEEE Trans Biomed Eng. 2001; 48:1347–1351. PMID: 11686634.
Article2. Choi KY, Kim GK, Lim YJ, Kim TS, Leem W, Rhee BA. Comparison of intraoperative somatosensory evoked potential (SSEP) monitoring during aneurysm surgery. J Korean Neurosurg Soc. 2001; 30(Suppl 2):S281–S288.3. Freye E. Cerebral monitoring in the operating room and the intensive care unit-an introductory for the clinician and a guide for the novice wanting to open a window to the brain. Part II : Sensory-evoked potentials (SS-EP, AEP, VEP). J Clin Monit Comput. 2005; 19:77–168. PMID: 16167223.
Article4. Fridman J, John ER, Bergelson M, Kaiser JB, Baird HW. Application of digital filtering and automatic peak detection to brain stem auditory evok-ed potential. Electroencephalogr Clin Neurophysiol. 1982; 53:405–416. PMID: 6175502.
Article5. Friedman WA, Chadwick GM, Verhoeven FJ, Mahla M, Day AL. Monitoring of somatosensory evoked potentials during surgery for middle cerebral artery aneurysms. Neurosurgery. 1991; 29:83–88. PMID: 1870692.
Article6. Goryawala M, Yaylali I, Cabrerizo M, Vedala K, Adjouadi M. An effective intra-operative neurophysiological monitoring scheme for aneurysm clipping and spinal fusion surgeries. J Neural Eng. 2012; 9:026021. PMID: 22419062.
Article7. Hu Y, Liu H, Luk KD. Time-frequency analysis of somatosensory evoked potentials for intraoperative spinal cord monitoring. J Clin Neurophysiol. 2011; 28:504–511. PMID: 21946365.
Article8. Husain AM. A Practical Approach to Neurophysiologic Intraoperative Monitoring. New York: Demos;2008.9. Kang D, Yao P, Wu Z, Yu L. Ischemia changes and tolerance ratio of evoked potential monitoring in intracranial aneurysm surgery. Clin Neurol Neurosurg. 2013; 115:552–556. PMID: 22795547.
Article10. Krayenbühl N, Sarnthein J, Oinas M, Erdem E, Krisht AF. MRI-validation of SEP monitoring for ischemic events during microsurgical clipping of intracranial aneurysms. Clin Neurophysiol. 2011; 122:1878–1882. PMID: 21377924.
Article11. Mizoi K, Yoshimoto T. Permissible temporary occlusion time in aneurysm surgery as evaluated by evoked potential monitoring. Neurosurgery. 1993; 33:434–440. discussion 440. PMID: 8413875.
Article12. Møller AR. Intraoperative neurophysiological monitoring. ed 3. New York: Springer;2011.13. Momma F, Wang AD, Symon L. Effects of temporary arterial occlusion on somatosensory evoked responses in aneurysm surgery. Surg Neurol. 1987; 27:343–352. PMID: 3824140.
Article14. Nave G, Eldar YC, Inbar G, Sinai A, Pratt H, Zaaroor M. Real-time change detection of steady-state evoked potentials. Biol Cybern. 2013; 107:49–59. PMID: 23053433.
Article15. Nuwer MR. Overview and history in Nuwer MR (ed) : Intraoperative Monitoring of Neural Function. Amsterdam: Elsevier;2008.16. Nuwer MR, Packwood JW. Somatosensory evoked potential monitoring with scalp and cervical recording in Nuwer MR (ed) : Intraoperative Monitoring of Neural Function. Amsterdam: Elsevier;2008.17. Penchet G, Arné P, Cuny E, Monteil P, Loiseau H, Castel JP. Use of intraoperative monitoring of somatosensory evoked potentials to prevent ischaemic stroke after surgical exclusion of middle cerebral artery aneurysms. Acta Neurochir (Wien). 2007; 149:357–357. PMID: 17380251.
Article18. Schick U, Döhnert J, Meyer JJ, Vitzthum HE. Effects of temporary clips on somatosensory evoked potentials in aneurysm surgery. Neurocrit Care. 2005; 2:141–149. PMID: 16159056.
Article19. Schramm J, Koht A, Schmidt G, Pechstein U, Taniguchi M, Fahlbusch R. Surgical and electrophysiological observations during clipping of 134 aneurysms with evoked potential monitoring. Neurosurgery. 1990; 26:61–70. PMID: 2294480.
Article20. Smith SW. The scientist and engineer's guide to digital signal processing. ed 2. San Diego: California Technical Publishing;1999.21. Symon L, Momma F, Murota T. Assessment of reversible cerebral ischaemia in man : intraoperative monitoring of the somatosensory evoked response. Acta Neurochir Suppl(Wien). 1988; 42:3–7. PMID: 3189017.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Neurophysiologic Monitoring: Basic Principles and Recent Update
- Intraoperative Monitoring for Tethered Cord Syndrome Using Somatosensory Evoked Potential and Motor Evoked Potential: Report of three cases
- Intraoperative Monitoring Using Somatosensory Evoked Potential during Spinal Deformity Surgery
- Intraoperative monitoring of somatosensory and visual evoked potentials for detecting posterior cerebral artery infarction during anteromesial temporal resection
- Intraoperative Neurophysiological Monitoring for Spinal Cord Tumor Surgery: Comparison of Motor and Somatosensory Evoked Potentials According to Tumor Types
