A Case of Intradural-Extramedullary Form of Primary Spinal Cysticercosis Misdiagnosed as an Arachnoid Cyst
- Affiliations
-
- 1Department of Neurosurgery, Spine Center, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. kijeong@snu.ac.kr
- KMID: 2191099
- DOI: http://doi.org/10.3340/jkns.2014.55.4.226
Abstract
- We describe a rare case of intradural-extramedullary primary spinal cysticercosis. A 42-year-old man visited our institute for lower back pain. He denied having consumed raw meet. Magnetic resonance (MR) images revealed an intradural pure cystic mass at the L3-L4 level. A radiologic diagnosis of spinal arachnoid cyst was established. Three years later, he complained of aggravated back pain, and follow-up MR examination showed a markedly expanded cyst, occupying the subarachnoid space from the T11 to the S1 level. L2 hemilaminectomy was performed, and a yellowish infected cyst bulged out through the dural opening. The cyst was removed en bloc. The histopathological findings of the cyst were consistent with parasitic infection. Serum enzyme-linked immunosorbent assay (ELISA) confirmed the presence of spinal cysticercosis. As there was no intracranial lesion, the final diagnosis was primary spinal cysticercosis, which is very rare. MR imaging is a sensitive diagnostic tool for detecting cystic lesions in the spine; however, it is difficult to distinguish cysticercosis from non-infectious cysts such as an arachnoid cyst without using gadolinium enhancement. Clinicians treating spinal cysts with an unusual clinical course should include cysticercosis as a differential diagnosis. We recommend contrast-enhanced MR imaging and serum ELISA in the diagnostic work-up of such cases.
MeSH Terms
Figure
-
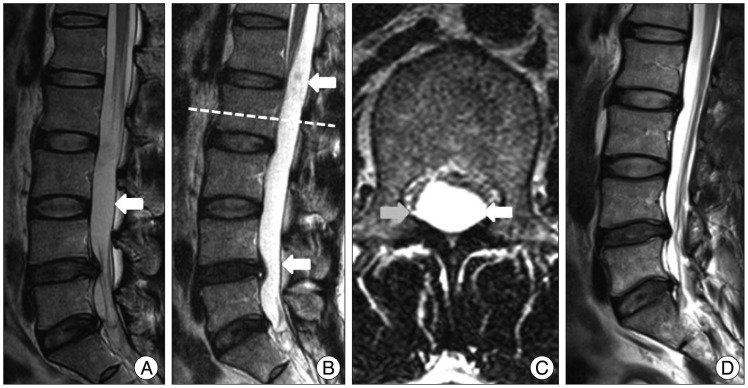
Fig. 1 Magnetic resonance imaging of the lumbar spine : Sagittal T2-weighted image showing an intradural cystic lesion (arrow) that is well circumscribed at the L3-L4 level (A). Three years later, follow-up sagittal (B) and axial (C) T2-weighted images of the L2 level reveal that the cyst (arrow) has grown, and occupies the T11-S1 levels. Post-operative images showing that the spinal cysticercosis has been removed without remnants (D).

Fig. 2 Intraoperative photographs showing the cystic lesion observed after opening the dura (asterisk). The removed cyst was an oval-shaped yellowish lesion.
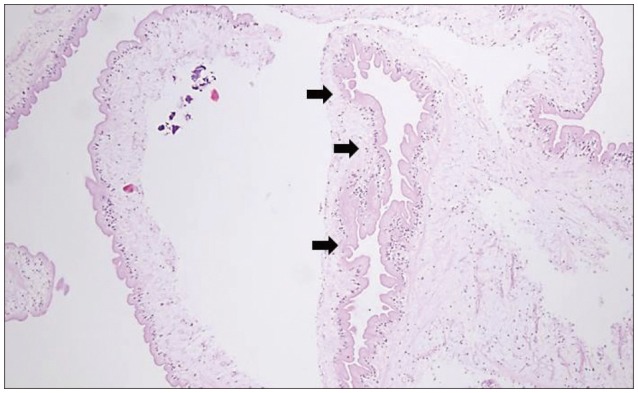
Fig. 3 Photomicrograph of the specimen showing a translucent cyst wall with eosinophilic lining (black arrows), and chronic inflammatory cells (Hematoxylin & Eosin, original magnification ×100).
Reference
-
1. Azfar SF, Kirmani S, Badar F, Ahmad I. Isolated intramedullary spinal cysticercosis in a 10-year-old female showing dramatic response with albendazole. J Pediatr Neurosci. 2011; 6:52–54. PMID: 21977090.2. Bustos JA, Pretell EJ, Llanos-Zavalaga F, Gilman RH, Del Brutto OH, Garcia HH, et al. Efficacy of a 3-day course of albendazole treatment in patients with a single neurocysticercosis cyst. Clin Neurol Neurosurg. 2006; 108:193–194. PMID: 16412842.
Article3. De Souza Queiroz L, Filho AP, Callegaro D, De Faria LL. Intramedullary cysticercosis. Case report, literature review and comments on pathogenesis. J Neurol Sci. 1975; 26:61–70. PMID: 1159459.4. Gupta S, Singh PK, Gupta B, Singh V, Azam A. Isolated primary intradural extramedullary spinal neurocysticercosis: a case report and review of literature. Acta Neurol Taiwan. 2009; 18:187–192. PMID: 19960962.5. Hawk MW, Shahlaie K, Kim KD, Theis JH. Neurocysticercosis : a review. Surg Neurol. 2005; 63:123–132. discussion 132. PMID: 15680651.6. Jang JW, Lee JK, Lee JH, Seo BR, Kim SH. Recurrent primary spinal subarachnoid neurocysticercosis. Spine (Phila Pa 1976). 35:2010; E172–E175. PMID: 20118838.
Article7. Jongwutiwes U, Yanagida T, Ito A, Kline SE. Isolated intradural-extramedullary spinal cysticercosis : a case report. J Travel Med. 2011; 18:284–287. PMID: 21722242.
Article8. Leite CC, Jinkins JR, Escobar BE, Magalhães AC, Gomes GC, Dib G, et al. MR imaging of intramedullary and intradural-extramedullary spinal cysticercosis. AJR Am J Roentgenol. 1997; 169:1713–1717. PMID: 9393195.
Article9. Mohanty A, Venkatrama SK, Das S, Das BS, Rao BR, Vasudev MK. Spinal intramedullary cysticercosis. Neurosurgery. 1997; 40:82–87. PMID: 8971828.
Article10. Nash TE, Neva FA. Recent advances in the diagnosis and treatment of cerebral cysticercosis. N Engl J Med. 1984; 311:1492–1496. PMID: 6390196.
Article11. Park YS, Lee JK, Kim JH, Park KC. Cysticercosis of lumbar spine, mimicking spinal subarachnoid tumor. Spine J. 2011; 11:e1–e5. PMID: 21474075.
Article12. Paterakis KN, Kapsalaki E, Hadjigeorgiou GM, Barbanis S, Fezoulidis I, Kourtopoulos H. Primary spinal intradural extramedullary cysticercosis. Surg Neurol. 2007; 68:309–311. discussion 312. PMID: 17719976.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- An Arachnoid Cyst in Cervical Spinal Canal: Case Report
- A Case of a Thoracic Spinal Intradural Arachnoid Cyst with Chest Pain
- Sacral Intradural Cysticercosis Misdiagnosed as Brain Tumor Metastasis
- Herniated Lumbar Disc Combined with Spinal Intradural Extramedullary Cysticercosis
- Intradural Extramedullary Cysticercosis Involving the Thoracolumbar Spinal Canal in a Patient with Cerebral Cysticercosis
