Necrotizing fasciitis of the head and neck: a case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, Wonkwang University School of Dentistry, Iksan, Korea. omschoi@wonkwang.ac.kr
- KMID: 2189471
- DOI: http://doi.org/10.5125/jkaoms.2015.41.2.90
Abstract
- Necrotizing fasciitis (NF) is an infection that spreads along the fascial planes, causing subcutaneous tissue death characterized by rapid progression, systemic toxicity, and even death. NF often appears as a red, hot, painful, and swollen wound with an ill-defined border. As the infective process continues, local pain is replaced by numbness or analgesia. As the disease process continues, the skin initially becomes pale, then mottled and purple, and finally, gangrenous. The ability of NF to move rapidly along fascial planes and cause tissue necrosis is secondary to its polymicrobial composition and the synergistic effect of the enzymes produced by the bacteria. Treatment involves securing the airway, broad-spectrum antimicrobial therapy, intensive care support, and prompt surgical debridement, repeated as needed. Reducing mortality rests on early diagnosis and prompt aggressive treatment.
MeSH Terms
Figure
-

Fig. 1 On clinical examination, the patient showed swollen and reddish skin in the submandibular, submental, and upper neck areas.

Fig. 2 Computed tomographies showed a disseminated deep neck space abscess in the left submandibular space that extended into the upper mediastinum through the anterior neck space and to the supraclavicular and axillary areas.

Fig. 3 Necrotic fascia was removed, and the infected area were drained. The fascia was fragile and discolored to grayish.

Fig. 4 An artificial airway was secured, and the area under the trapezius muscle was drained.
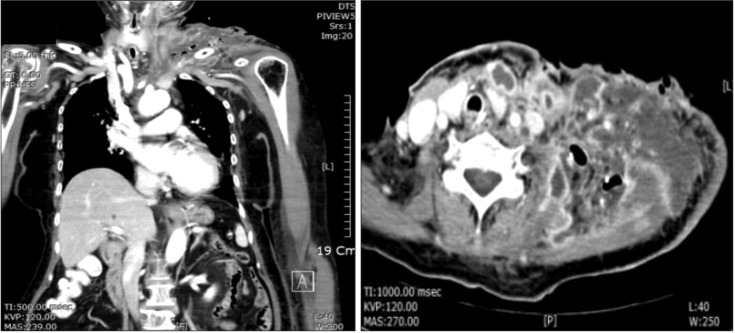
Fig. 5 Deterioration of the multifocal abscess around the left chest wall, shoulder area, and carotid area.
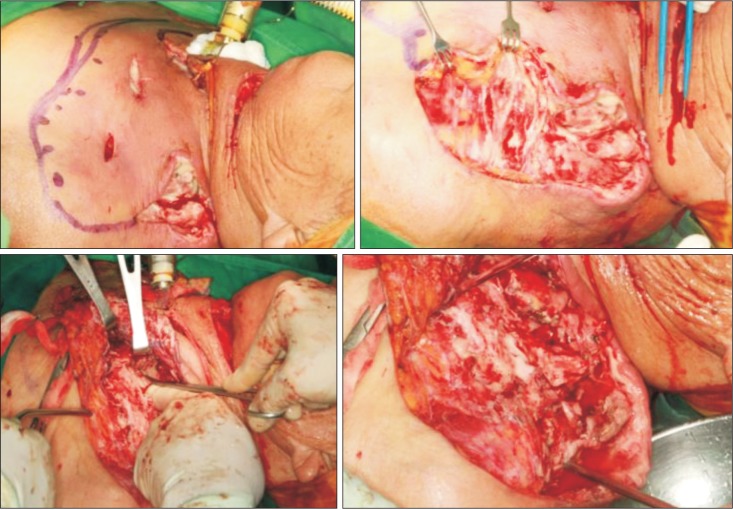
Fig. 6 After skin elevation, all necrotic fascia were exposed. We performed fasciotomy with fingers and scissors around the upper chest and carotid and shoulder areas.
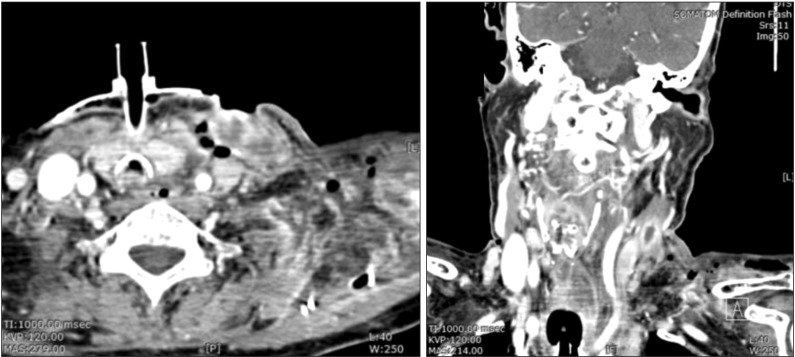
Fig. 7 Markedly decreased infection state.

Fig. 8 After the infection subsided, the shoulder skin was not salvagable. The defect was closed with bilobed rotational flap.
Reference
-
1. Wilson B. Necrotizing fasciitis. Am Surg. 1952; 18:416–431. PMID: 14915014.2. Green RJ, Dafoe DC, Raffin TA. Necrotizing fasciitis. Chest. 1996; 110:219–229. PMID: 8681631.
Article3. Stamenkovic I, Lew PD. Early recognition of potentially fatal necrotizing fasciitis. The use of frozen-section biopsy. N Engl J Med. 1984; 310:1689–1693. PMID: 6727947.4. Puvanendran R, Huey JC, Pasupathy S. Necrotizing fasciitis. Can Fam Physician. 2009; 55:981–987. PMID: 19826154.5. Hefny AF, Eid HO, Al-Hussona M, Idris KM, Abu-Zidan FM. Necrotizing fasciitis: a challenging diagnosis. Eur J Emerg Med. 2007; 14:50–52. PMID: 17198329.
Article6. Lee JW, Immerman SB, Morris LG. Techniques for early diagnosis and management of cervicofacial necrotising fasciitis. J Laryngol Otol. 2010; 124:759–764. PMID: 20298644.
Article7. Quereshy FA, Baskin J, Barbu AM, Zechel MA. Report of a case of cervicothoracic necrotizing fasciitis along with a current review of reported cases. J Oral Maxillofac Surg. 2009; 67:419–423. PMID: 19138621.
Article8. Maisel RH, Karlen R. Cervical necrotizing fasciitis. Laryngoscope. 1994; 104:795–798. PMID: 8022239.
Article9. Kantu S, Har-El G. Cervical necrotizing fasciitis. Ann Otol Rhinol Laryngol. 1997; 106:965–970. PMID: 9373088.
Article10. Lin C, Yeh FL, Lin JT, Ma H, Hwang CH, Shen BH, et al. Necrotizing fasciitis of the head and neck: an analysis of 47 cases. Plast Reconstr Surg. 2001; 107:1684–1693. PMID: 11391186.
Article11. Weiss A, Nelson P, Movahed R, Clarkson E, Dym H. Necrotizing fasciitis: review of the literature and case report. J Oral Maxillofac Surg. 2011; 69:2786–2794. PMID: 21367503.
Article12. Schütz P, Joshi RM, Ibrahim HHH. Odontogenic necrotizing fasciitis of the neck and upper chest wall. J Oral Maxillofac Surg Med Pathol. 2012; 24:32–35.
Article13. Peterson LJ. Principles of oral and maxillofacial surgery. Philadelphia, PA: Lippincott;1992. p. 184–188.14. Tung-Yiu W, Jehn-Shyun H, Ching-Hung C, Hung-An C. Cervical necrotizing fasciitis of odontogenic origin: a report of 11 cases. J Oral Maxillofac Surg. 2000; 58:1347–1352. PMID: 11117681.
Article15. Becker M, Zbären P, Hermans R, Becker CD, Marchal F, Kurt AM, et al. Necrotizing fasciitis of the head and neck: role of CT in diagnosis and management. Radiology. 1997; 202:471–476. PMID: 9015076.
Article16. Richardson D, Schmitz JP. Chronic relapsing cervicofacial necrotizing fasciitis: case report. J Oral Maxillofac Surg. 1997; 55:403–408. PMID: 9120705.
Article17. Shindo ML, Nalbone VP, Dougherty WR. Necrotizing fasciitis of the face. Laryngoscope. 1997; 107:1071–1079. PMID: 9261011.
Article18. Ord R, Coletti D. Cervico-facial necrotizing fasciitis. Oral Dis. 2009; 15:133–141. PMID: 19207484.
Article
