Shoulder Operation
- Affiliations
-
- 1Department of Orthopaedic Surgery/Shoulder, Elbow and Sports Service, Konkuk University College of Medicine, Korea. drpark@chol.com
- KMID: 2188056
- DOI: http://doi.org/10.5124/jkma.2009.52.8.795
Abstract
- Although shoulder pain is a very common problem and compromised shoulder movement due to pain, stiffness, or weakness can cause substantial disability, many patients fail to recognize a need for a proper treatment. The diagnosis and treatment of the shoulder should be specified for each of the disease entity. Most of shoulder pain can be managed non-operatively with a well-organized rehabilitation program. However, the surgery should always remain as an option in case of failure of conservative managements, which can be seen from a definite indication of a patient's condition. The article presents four representative disease entities other than shoulder trauma occurring in old age which doctors see most often at outpatient's clinics. Impingement syndrome, rotator cuff tear, calcifying tendonitis, and arthritis are described in this article, introducing each diseases and surgical indications and descriptions, and their results.
Figure
-
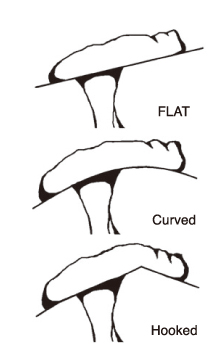
Figure 1 Type I: Flat Acromion, Type II: Curved Acromion, Type III: Hooked Acromion
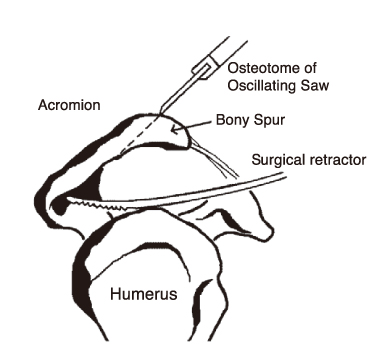
Figure 2 Acromioplasty-Cutting anterior subacromial spur and flattening undersurface of the acromion. Also Coracoacromial Ligament is released.
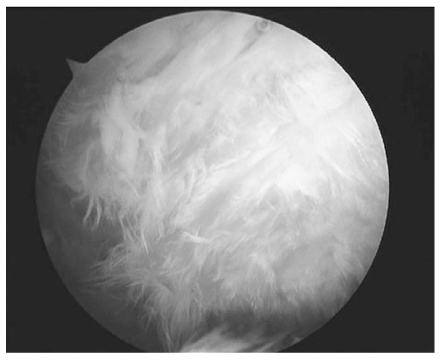
Figure 3 Fraying of the undersurface of the acromion.

Figure 4 Subacromial spur seen from arthroscopic camera.
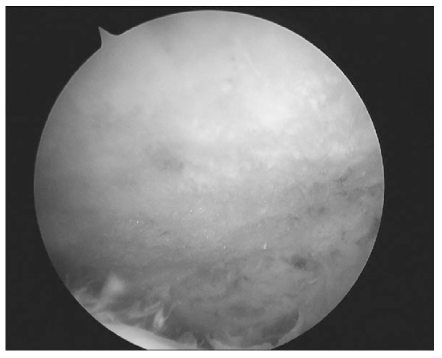
Figure 5 Flattened subacromial undersurface after arthroscopic acromioplasty.

Figure 6 Rotator cuff tear identified during minimal open rotator cuff repair.

Figure 7 Rotator cuff is sutured and ready to pull laterally.

Figure 8 Rotator cuff repair is done.
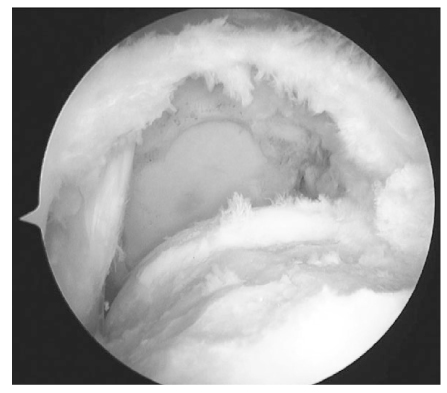
Figure 9 Rotator cuff tear seen from arthroscopic camera.
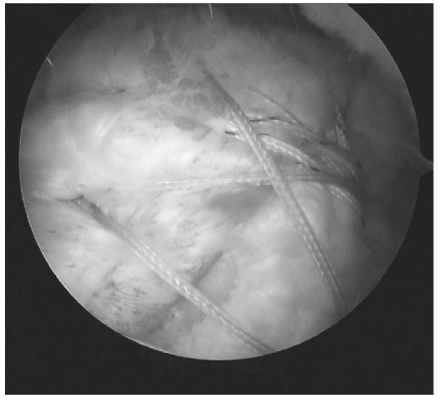
Figure 10 Rotator cuff repair done through arthroscopic technique.

Figure 11 Simple X-ray showing calcific tendonitis.
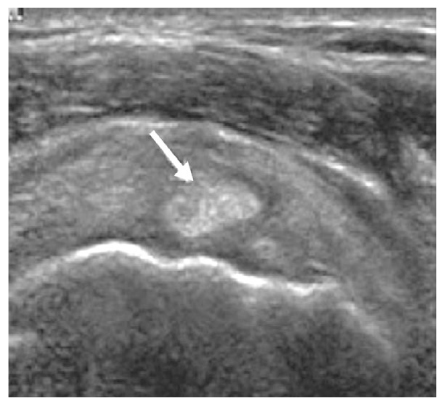
Figure 12 Ultrasound shoing calcific tendonitis.
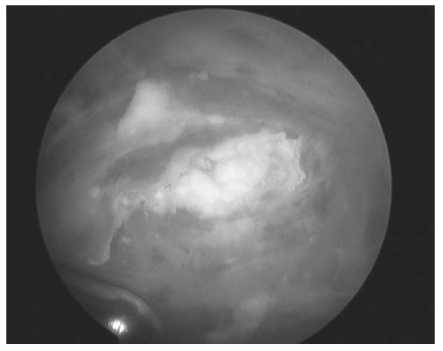
Figure 13 Calcific deposit found on bursal side of supraspinatus tendon through arthroscopic examination.
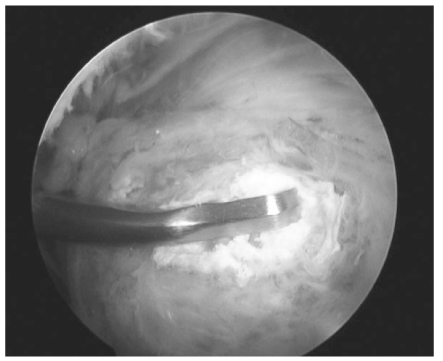
Figure 14 Calcific deposit being removed.
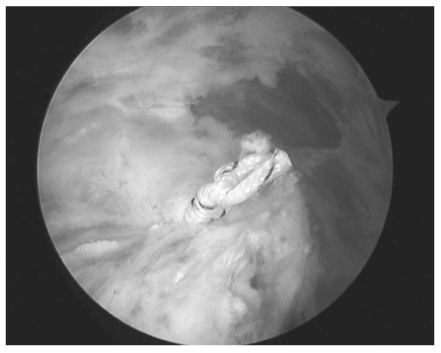
Figure 15 Repair of the supraspinatus tendon after removal of the calcific deposit.

Figure 16 Simple X-ray of shoulder osteoarthritis.

Figure 17 Post-operative simple X-ray after total shoulder arthroplasty.

Figure 18 Simple X-ray sho-wing cuff tear arthropathy.

Figure 19 Simple X-ray showing reverse shoulder arthroplasty.
Cited by 2 articles
-
Update in surgical treatment of shoulder injuries
Sang-Hoon Lhee, Moon Sang Chung, Jeong Suh Kim, Do Young Lee
J Korean Med Assoc. 2014;57(8):667-678. doi: 10.5124/jkma.2014.57.8.667.The Size of the Rotator Cuff and the Positional Relationship of Bony Landmarks: An Anatomical Study
Gyeong-Jin Kim, Ho-Jung Cho, Yong-Seok Nam, Seung-Ho Han, In-Beom Kim
Korean J Phys Anthropol. 2015;28(1):11-17. doi: 10.11637/kjpa.2015.28.1.11.
Reference
-
1. Cummins CA, Sasso LM, Nicholson D. Impingement syndrome: temporal outcomes of nonoperative treatment. J Shoulder Elbow Surg. 2009. 18:172–177.
Article2. Neer CS 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am. 1972. 54:41–50.
Article3. Chin PY, Sperling JW, Cofield RH, Stuart MJ, Crownhart BS. Anterior acromioplasty for the shoulder impingement syndrome: long-term outcome. J Shoulder Elbow Surg. 2007. 16:697–700.
Article4. Odenbring S, Wagner P, Atroshi I. Long-term outcomes of arthroscopic acromioplasty for chronic shoulder impingement syndrome: a prospective cohort study with a minimum of 12 years' follow-up. Arthroscopy. 2008. 24:1092–1098.
Article5. Stephens SR, Warren RF, Payne LZ, Wickiewicz TL, Altchek DW. Arthroscopic acromioplasty: a 6-to 10-year follow-up. Arthroscopy. 1998. 14:382–388.6. Bartolozzi A, Andreychik D, Ahmad S. Determinants of outcome in the treatment of rotator cuff disease. Clin Orthop Relat Res. 1994. 11. 308:90–97.
Article7. Ellman H, Hanker G, Bayer M. Repair of the rotator cuff. Endresult study of factors influencing reconstruction. J Bone Joint Surg Am. 1986. 68:1136–1144.
Article8. Frost P, Andersen JH, Lundorf E. Is supraspinatus pathology as defined by magnetic resonance imaging associated with clinical sign of shoulder impingement? J Shoulder Elbow Surg. 1999. 8:565–568.
Article9. Milgrom C, Schaffler M, Gilbert S, van Holsbeeck M. Rotatorcuff changes in asymptomatic adults. The effect of age, hand dominance and gender. J Bone Joint Surg Br. 1995. 77:296–298.
Article10. Sher JS, Uribe JW, Posada A, Murphy BJ, Zlatkin MB. Abnormal findings on magnetic resonance images of asymptomatic shoulders. J Bone Joint Surg Am. 1995. 77:10–15.
Article11. Gerber C, Meyer DC, Schneeberger AG, Hoppeler H, von Rechenberg B. Effect of tendon release and delayed repair on the structure of the muscles of the rotator cuff: an experimental study in sheep. J Bone Joint Surg Am. 2004. 86-A:1973–1982.12. Morse K, Davis AD, Afra R, Kaye EK, Schepsis A, Voloshin I. Arthroscopic versus mini-open rotator cuff repair: a comprehensive review and meta-analysis. Am J Sports Med. 2008. 36:1824–1828.13. Millar NL, Wu X, Tantau R, Silverstone E, Murrell GA. Open versus two forms of arthroscopic rotator cuff repair. Clin Orthop Relat Res. 2009. 467:966–978.
Article14. Youm T, Murray DH, Kubiak EN, Rokito AS, Zuckerman JD. Arthroscopic versus mini-open rotator cuff repair: a comparison of clinical outcomes and patient satisfaction. J Shoulder Elbow Surg. 2005. 14:455–459.
Article15. Park JY, Chung KT, Yoo MJ. A serial comparison of arthroscopic repairs for partial- and full-thickness rotator cuff tears. Arthroscopy. 2004. 20:705–711.
Article16. Park JY, Lhee SH, Choi JH, Park HK, Yu JW, Seo JB. Comparison of the clinical outcomes of single -and doublerow repairs in rotator cuff tears. Am J Sports Med. 2008. 36:1310–1316.
Article17. Ark JW, Flock TJ, Flatow EL, Bigliani LU. Arthroscopic treatment of calcific tendinitis of the shoulder. Arthroscopy. 1992. 8:183–188.
Article18. Jerosch J, Strauss JM, Schmiel S. Arthroscopic treatment of calcific tendinitis of the shoulder. J Shoulder Elbow Surg. 1998. 7:30–37.
Article19. Re LP Jr, Karzel RP. Management of rotator cuff calcifications. Orthop Clin North Am. 1993. 24:125–132.
Article20. Seil R, Litzenburger H, Kohn D, Rupp S. Arthroscopic treatment of chronically painful calcifying tendinitis of the supraspinatus tendon. Arthroscopy. 2006. 22:521–527.
Article21. Cuomo F, Checroun A. Avoiding pitfalls and complications in total shoulder arthroplasty. Orthop Clin North Am. 1998. 29:507–518.
Article22. van de Sande MA, Brand R, Rozing PM. Indications, complications, and results of shoulder arthroplasty. Scand J Rheumatol. 2006. 35:426–434.
Article23. Wirth MA, Rockwood CA Jr. Complications of total shoulder-replacement arthroplasty. J Bone Joint Surg Am. 1996. 78:603–616.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Treatment of Recurrent Anterior Dislocation of the Shoulder by Bristow Operation
- The Treatment of Recurrent Anterior Dislocation of the Shoulder by Modified Bristow Operation
- A 14 Cases of Recurrent Shoulder Dislocation Treated by Modified Bristow Operation
- The Result of Modified Bankart Operation with Suture Anchor in Traumatic Recurrent Anterior Dislocation of Shoulder Joint
- Combinded Bankart and Putti-Platt operation for the anterior recurrent dislocation of shoulder
