Esophageal Fistula Formation by MetalLoosening following Anterior Cervical Arthrodesis: A Case Report
- Affiliations
-
- 1Department of Orthopaedic Surgery, College of Medicine, Research Institute of Clinical Medicine, Chonbuk National University Hospital, Jeonju, Korea. kysong@chonbuk.ac.kr
- KMID: 2186568
- DOI: http://doi.org/10.4055/jkoa.2007.42.3.404
Abstract
- An esophageal injury after an anterior cervical discectomy and fusion with plating is a well known but a fatal complication. If the diagnosis is delayed, inflammation can spread out into the neighboring main organs resulting in a very poor prognosis despite vigorous treatment. We report a case of esophageal fistula formation as a result of infected metal loosening after an anterior cervical discectomy and fusion with plating, which was treated successfully with a satisfactory clinical outcome.
Figure
-
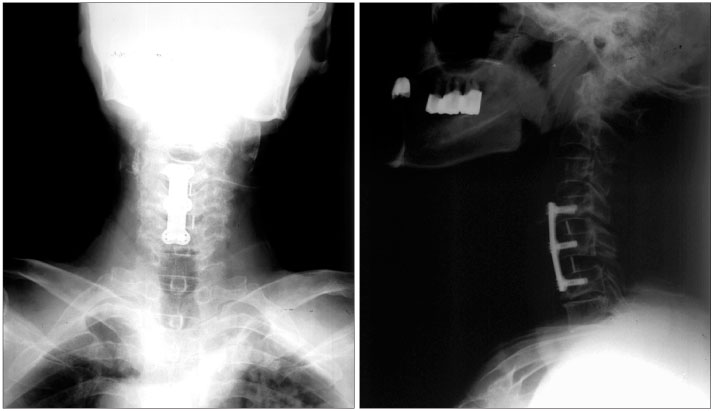
Fig. 1 Radiographs immediately after the index operation at a local clinic shows a normal sagittal alignment with cages and plate in the correct position.
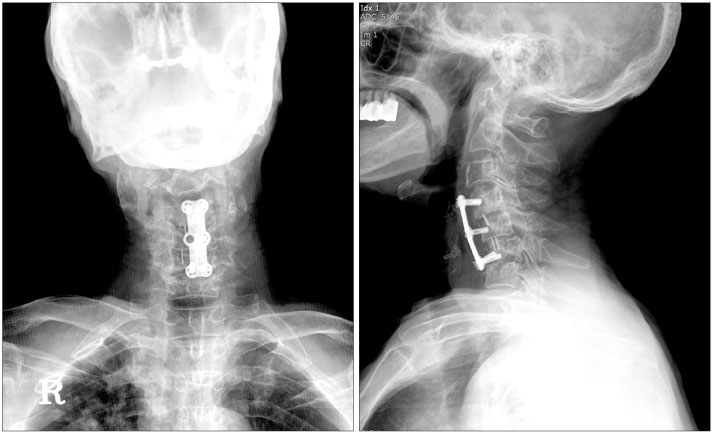
Fig. 2 Radiographs 8 months after the index operation; back-out of screws, one screw lost after the index surgery with suspicious infectious loosening. The white arrow indicates gas in the pouch at the midportion of the plate.

Fig. 3 Follow-up radiograph of plain film at the secondary visit. Radiographs 18 months after the index operation; back-out of screws, another screw lost after the index surgery and progressive infectious loosening. The white arrow indicates gas in the pouch at the lower part of the plate.
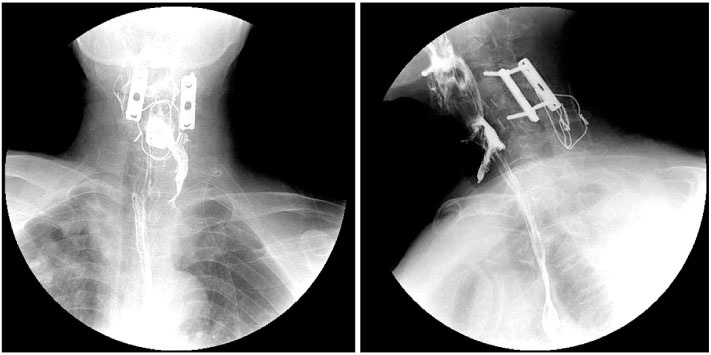
Fig. 4 Initial esophagogram taken 8 days after revision surgery. An approximately 6 mm sized esophageal fistula in esophagopharyngeal junction and an approximately 7 cm sized barium collection in the left sided paraesophageal region.
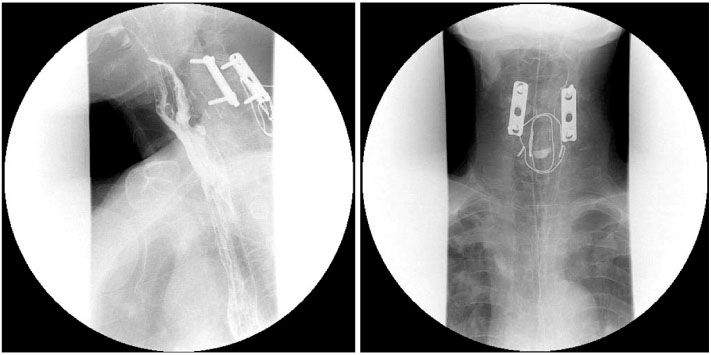
Fig. 5 Follow-up esophagogram taken 4 weeks after Levintube insertion. The esophageal fistula size had decreased and was approximately 1.8 cm in size lined pouch located at the esophagopharyngeal junction site.
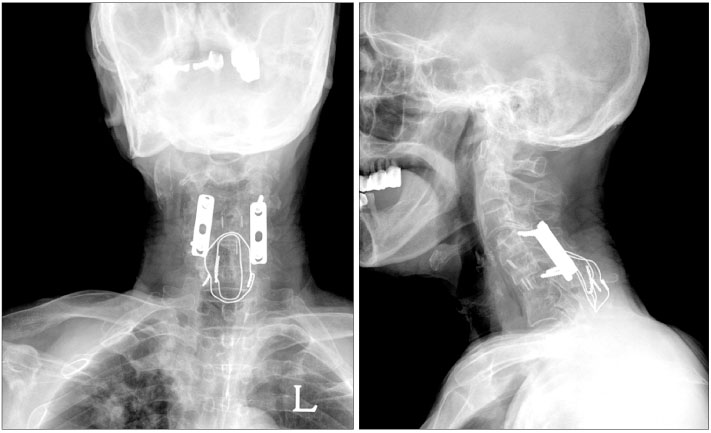
Fig. 6 Last follow-up plain radiographs showing solid fusion with a normal sagittal alignment 12 months after revision surgery.
Reference
-
1. Capen DA, Garland DE, Waters RL. Surgical stabilization of the cervical spine. A comparative analysis of anterior and posterior spine fusions. Clin Orthop Relat Res. 1985. 196:229–237.
Article2. Gaudinez RF, English GM, Gebhard JS, Brugman JL, Donaldson DH, Brown CW. Esophageal perforations after anterior cervical surgery. J Spinal Disord. 2000. 13:77–84.
Article3. Jones WG 2nd, Ginsberg RJ. Esophageal perforation: a continuing challenge. Ann Thorac Surg. 1992. 53:534–543.
Article4. Tew JM Jr, Mayfield FH. Complications of surgery of the anterior cervical spine. Clin Neurosurg. 1976. 23:424–434.
Article5. Yee GK, Terry AF. Esophageal penetration by an anterior cervical fixation device. A case report. Spine. 1993. 18:522–527.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Esophageal Fistula Related to Anterior Cervical Spine Surgery after Severe Cervical Trauma
- A Case of Pharyngoesophageal Diverticulum (Zenker's Diverticulum) Following Anterior Cervical Spine Screw or Plate Fixation
- Anterior Fusion with Corpectomy and Autogenous Iliac Graft for Cervical Kyphosis in Neurofibromatosis: A case report
- Surgical Treatment of Esophago-Cutaneous Fistula Developing after Anterior Cervical Spine Surgery: Case Report
- A Case of the Esophageal Atresia with Distal Tracheoesophageal Fistula Associated with Duodenal Obstrction
