Recalcitrant Lateral Epicondylitis: Open and Arthroscopic Release
- Affiliations
-
- 1Department of Orthopedic Surgery, Gil Medical Center, Gachon University, Inchon, Korea. kykhyr@gilhospital.com
- KMID: 2186454
- DOI: http://doi.org/10.4055/jkoa.2008.43.3.366
Abstract
-
PURPOSE: To compare clinical outcomes when using open or arthroscopic release for recalcitrantlateral epicondylitis.
MATERIALS AND METHODS
A total of 34 cases were followed up for an average of 16 months. Open release was performed in 21, and arthroscopic release in 13. In the open release group, arthroscopic examination was performed first in 7. Intraarticular and extraarticular lesions of the extensor tendon were compared. Pain was evaluated using the Visual Analog Scale, and function was evaluated using the assessment of Nirschl and Pettrone.
RESULTS
In arthroscopic findings, 6 out of 20 cases were nearly normal, 6 showed fraying, 4 a linear tear, and 4 avulsion. Some (3 of 5) cases with nearly normal arthroscopic findings had mucinoid degeneration detected during the open procedure. Overall, 86% of open release and 85% of arthroscopic release showed satisfactory results.
CONCLUSION
The extraarticular and intraarticular surfaces of the extensor origin had diverse appearances, and both procedures showed satisfactory results. Therefore, arthroscopic release is a useful treatment option for recalcitrant lateral epicondylitis.
Figure
-
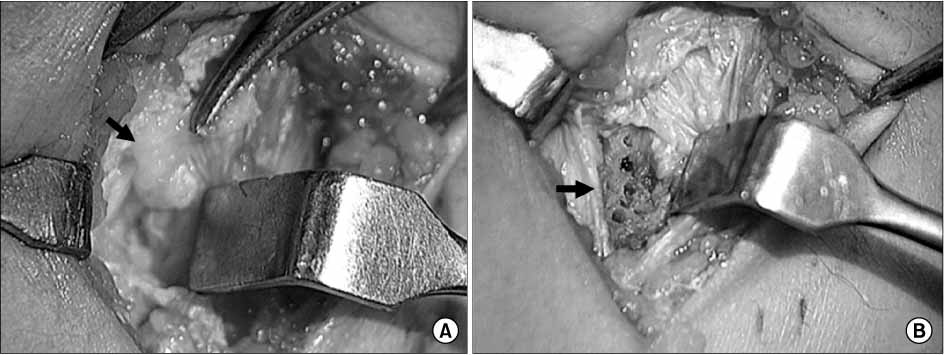
Fig. 1 Open procedure for recalcitrant lateral epicondylitis. (A) Pathologic tissue with mucinoid degeneration and the avulsion rupture of the extensor brevis origin (arrow) is carefully identified and resected. (B) The lateral epicondyle (arrow) is then drilled to enhance revascularization of the area.
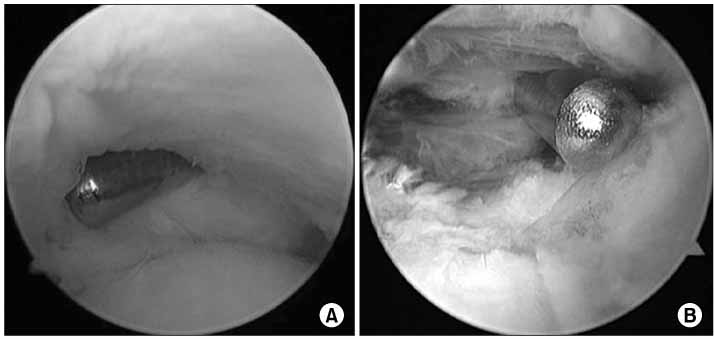
Fig. 2 Arthroscopic procedure for recalcitrant lateral epicondylitis. (A) The origin of the extensor brevis tendon is released arthroscopically. (B) Then, decortication of the lateral epicondyle is performed.
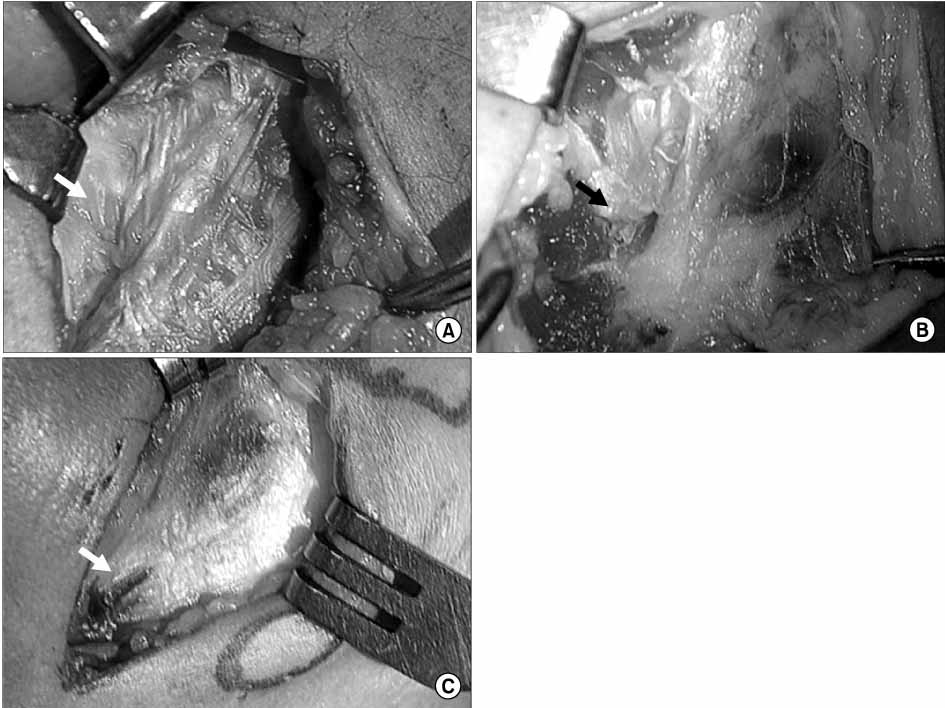
Fig. 3 Gross findings of extraarticular pathology of the extensor carpi radialis brevis tendon were classified into three types: (A) Mucinoid degeneration of the tendon with discolored tissue (type I), (B) Partial tear of the tendon (type II), (C) Complete tear of the tendon (type III).
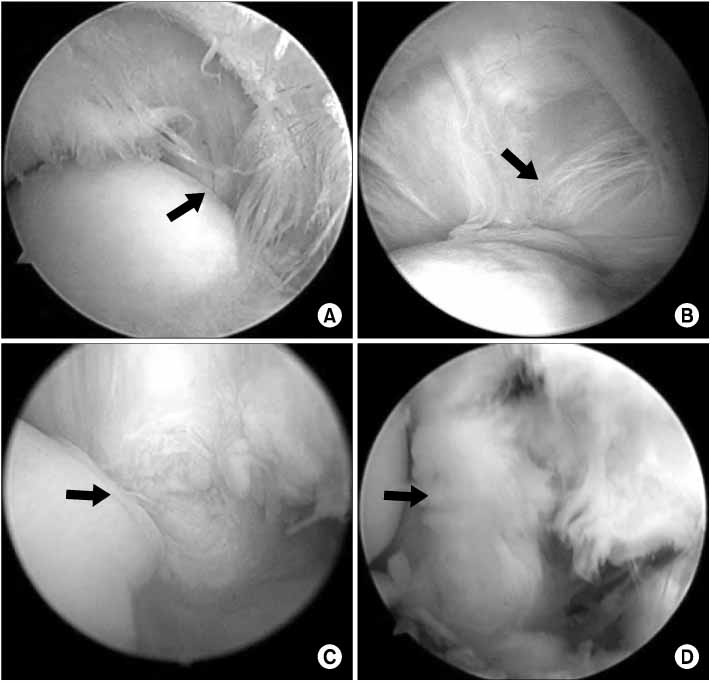
Fig. 4 Lesions on the undersurface of the extensor carpi radialis brevis tendon were classified using to the classification system proposed by Baker. (A) Fraying of the undersurface of the tendon without torn capsule (type I), (B) Linear tear in the capsule and tendon (type II), (C) Partial avulsion of the tendon (type IIIa), (D) Complete avulsion of the tendon (type IIIb).
Reference
-
1. Baker CL Jr, Murphy KP, Gottlob CA, Curd DT. Arthroscopic classification and treatment of lateral epicondylitis: two-year clinical results. J Shoulder Elbow Surg. 2000. 9:475–482.
Article2. Boyd HB, McLeod AC Jr. Tennis elbow. J Bone Joint Surg Am. 1973. 55:1183–1187.
Article3. Coonrad RW, Hooper WR. Tennis elbow: its course, natural history, conservative and surgical management. J Bone Joint Surg Am. 1973. 55:1177–1182.4. Field LD, Altchek DW, Warren RF, O'Brien SJ, Skyhar MJ, Wickiewicz TL. Arthroscopic anatomy of the lateral elbow: a comparison of three portals. Arthroscopy. 1994. 10:602–607.
Article5. Goldberg EJ, Abraham E, Siegal I. The surgical treatment of chronic lateral humeral epicondylitis by common extensor release. Clin Orthop Relate Res. 1988. 233:208–212.
Article6. Grifka J, Boenke S, Krämer J. Endoscopic therapy in epicondylitis radialis humeri. Arthroscopy. 1995. 11:743–748.
Article7. Jobe FW, Ciccotti MG. Lateral and medial epicondylitis of the elbow. J Am Acad Orthop Surg. 1994. 2:1–8.
Article8. Kraushaar BS, Nirschl RP. Tendinosis of the elbow (tennis elbow). Clinical features and findings of histological, immunohistochemical, and electron microscopy studies. J Bone Joint Surg Am. 1999. 81:259–278.9. Kuklo TR, Taylor KF, Murphy KP, Islinger RB, Heekin RD, Baker CL Jr. Arthroscopic release for lateral epicondylitis: a cadaveric model. Arthroscopy. 1999. 15:259–264.
Article10. Leach RE, Miller JK. Lateral and medial epicondylitis of the elbow. Clin Sports Med. 1987. 6:259–272.
Article11. Maiotti M, Bollanti A, Massoni C, editors. Arthroscopic release of common extensor tendon to treat chronic lateral epicondylitis. Presented at 24th annual meeting, Arthroscopy Association of North America. 2005. Vancouver.12. Mullett H, Sprague M, Brown G, Hausman M. Arthroscopic treatment of lateral epicondylitis: clinical and cadaveric studies. Clin Orthop Relat Res. 2005. 439:123–128.13. Nirschl RP, Pettrone FA. Tennis elbow. The surgical treatment of lateral epicondylitis. J Bone Joint Surg Am. 1979. 61:832–839.
Article14. Owens BD, Murphy KP, Kuklo TR. Arthroscopic release for lateral epicondylitis. Arthroscopy. 2001. 17:582–587.
Article15. Peart RE, Strickler SS, Schweitzer KM Jr. Lateral epicondylitis: a comparative study of open and arthroscopic lateral release. Am J Orthop. 2004. 33:565–567.16. Regan W, Wold LE, Coonrad R, Morrey BF. Microscopic histopathology of chronic refractory lateral epicondylitis. Am J Sports Med. 1992. 20:746–749.
Article17. Safran MR, editor. Arthroscopic management of lateral epicondylitis. Instr course lect at 23rd annual meeting, Arthroscopy Association of North America. 2004. Orlando. 376–378.18. Savoie FH, Field LD, Szabo SJ, editors. Lateral epicondylitis: An evaluation of three methods of operative treatment. Presented at 23rd annual meeting, Arthroscopy Association of North America. 2004. Orlando.19. Smith AM, Castle JA, Ruch DS. Arthroscopic resection of the common extensor origin: anatomic considerations. J Shoulder Elbow Surg. 2003. 12:375–379.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recent Updates on the Treatment of Lateral Epicondylitis
- Treatment of Recalcitrant Medial and Lateral Epicondylitis with Autologous Platelet Rich Plasma; Preliminary Report
- Lateral Epicondylitis: Current Concept
- Current Trends for Treating Lateral Epicondylitis
- Clinical Outcomes of Arthroscopic Debridement for Lateral Epicondylitis with Partial Injury of the Lateral Collateral Ligament Complex
