Pilonidal Cysts Occurring in the Sacrococcygeal Region and that were Misdiagnosed as a Simple Abscess
- Affiliations
-
- 1Department of Orthopedic Surgery, Soonchunhyang University College of Medicine, Cheonan, Korea. chhong@sch.ac.kr
- KMID: 2185602
- DOI: http://doi.org/10.4055/jkoa.2010.45.1.97
Abstract
- A pilonidal cyst is known to be a recurrent infectious disease in the sacrococcygeal region and it usually affects adolescents and adults. It is often misdiagnosed as a simple abscess or a sebaceous cyst, so there are many patients with pilonidal cysts who have gone through several operations. Although many treatments for this malady have been reported, the principle treatment for pilonidal cysts is radical excision. We report here on two cases of pilonidal cyst and the patients were misdiagnosed as having a simple abscess. We planned to perform incision and drainage, but the lesions were finally diagnosed as pilonidal cysts and so we performed radical excision for the treatment. We also review the medical literature on abscesses that occur in the sacrococcygeal region in early adulthood.
MeSH Terms
Figure
-

Figure 1 (A) T2WI sagittal view, an ovoid-shaped mass like lesion which is located in the subcutaneous fat layer, sacrum level is seen, which displays high signal intensity. (B) It displays iso-signal intensity at T1WI sagittal view. (C) It displays septal-like enhancement and central low signal intensity at Gd T1WI (However, it does not seem to invade the connected muscle and it is not seen the abnormal signal intensity at bone marrow, spinal canal and disc.).

Figure 2 When the patient visited hospital, pilonidal sinus was detected at 5 cm upper from the anus during the inspection.
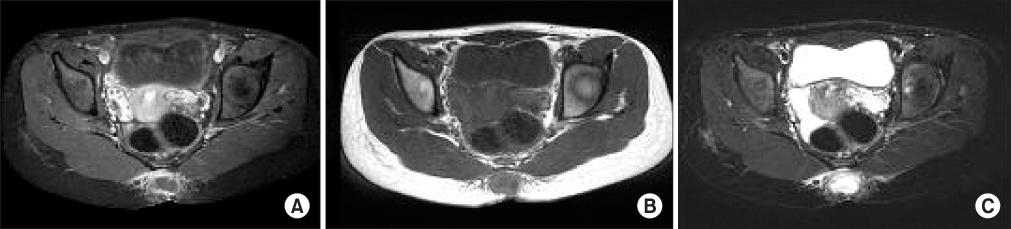
Figure 3 (A) T2WI axial view, a high signal intensity mass-like lesion is seen at the posterior aspect of coccyx, which displays peripheral thin-walled rim. (B) T1WI view, it displays low signal intensity. (C) Gd T1WI, the peripheral thin-walled rim is enhanced well.

Figure 4 This is photographed after total stitch out followed the radical resection operation.
Cited by 1 articles
-
Wide Excision Using Indigo-Carmine to Minimize the Recurrence of a Pilonidal Cyst: Technical Note
Chang-Hwa Hong, Woo-Jong Kim, Hak-Soo Kim
J Korean Orthop Assoc. 2019;54(2):197-202. doi: 10.4055/jkoa.2019.54.2.197.
Reference
-
1. Hegele A, Strombach FJ, Schönbach F. Reconstructive surgical therapy of infected pilonidal sinus. Chirurg. 2003. 74:749–752.2. Akinci OF, Coskun A, Uzunköy A. Simple and effective surgical treatment of pilonidal sinus: asymmetric excision and primary closure using suction drain and subcuiticular skin closure. Dis Colon Rectum. 2000. 43:701–707.3. Holmes LB, Turner EA Jr. Hereditary pilonidal sinus. JAMA. 1969. 209:1525–1526.
Article4. Chamberlain JW, Vawter GF. The congenital origin of pilonidal sinus. J Pediatr Surg. 1974. 9:441–444.
Article5. Karydakis GE. The etiology of pilonidal sinus. Hellenic Arm Forc Med Rev. 1975. 7:411–416.6. Allen-Mersh TG. Pilonidal sinus: finding the right tract for treatment. Br J Surg. 1990. 77:123–132.7. Buie LA. Jeep disease. South Med J. 1944. 37:103–109.
Article8. Karydakis GE. Hair insertion (pilonidal sinus). Hellenic Arm Forc Med Rev. 1968. 2:273–285.9. Karydakis GE. Easy and successful treatment of pilonidal sinus after explanation of its causative process. AUST N Z J Surg. 1992. 62:385–389.
Article10. Bascom JU. Pilonidal sinus. Curr Pract Surg. 1994. 6:175–180.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Wide Excision Using Indigo-Carmine to Minimize the Recurrence of a Pilonidal Cyst: Technical Note
- Pilonidal Abscess Associated With Primary Actinomycosis
- Surgical Treatment of Sacrococcygeal Pilonidal Sinus with a Leaf Flap
- Two Cases of Pilonidal Sinus
- Unroofing curettage for treatment of simple and complex sacrococcygeal pilonidal disease
