Arthroscopic Treatment of Femoroacetabular Impingement in Young Taekwondo Players
- Affiliations
-
- 1Department of Orthopedic Surgery, Chungnam National University School of Medicine, Daejeon, Korea. dshwang@cnu.ac.kr
- 2Department of Orthopedic Surgery, Bumin Hospital, Seoul, Korea.
- 3Department of Orthopedic Surgery, Konyang University College of Medicine, Daejeon, Korea.
- KMID: 2185428
- DOI: http://doi.org/10.4055/jkoa.2011.46.4.303
Abstract
- PURPOSE
We wanted to evaluate the clinical results and the radiological and arthroscopic findings of femoroacetabular impingement (FAI) in young Taekwondo players and to investigate the rate of returning-to-play Taekwondo and the recurrence rate.
MATERIALS AND METHODS
Twenty Taekwondo players (16 males and, 4 females) who were arthroscopically treated for FAI from September 2003 to July 2008 were retrospectively analyzed. Their mean age was 21.6 years old (range: 17 to 32 years) and the mean follow up was 33.7 months (range: 24 to 71 months). Plain radiographs and 3 dimensional computed tomography were taken in all patients and magnetic resonance arthrography was performed in 11 with suspicious soft tissue lesions. Labral injury, cartilage injury and associated lesions were evaluated by arthroscopy. The preoperative and postoperative visual analogue scale (VAS), the modified Harris hip score (MHHS), the sports frequency score (SFS), and the non-arthritic hip score (NAHS) were compared. We investigated the rate of returning-to-play at postoperative 1 year and at postoperative 2 years and the recurrence rate within 2 years after surgery.
RESULTS
There were 10 cam types, 1 pincer type and 9 mixed types. The mean alpha angle improved from 65.8 degrees preoperatively to 43.2 degrees postoperatively (p<0.001). Acetabular labral tears were accompanied in all cases and the most common tear site and type were at 2 o'clock and degenerative tear, respectively. In descending order, the acetabular cartilage injuries were located in the anterosuperior, posteroinferior and anterior portion, respectively. The femoral cartilage injuries were mostly located in the anterosuperior portion. The range of motion at the final follow-up showed improvement in all except abduction (p=0.262). The VAS, MHHS and SFS showed statistically significant improvement (p<0.001). The NAHS was improved, but without statistical significance (p=0.31). The rates of returning-to-play at postoperative 1 year and postoperative 2 years were 85% (17/20) and 75% (15/20), respectively. The recurrence rate within postoperative 2 years was 15% (3/20).
CONCLUSION
As screening test for FAI in young Taekwondo players is necessary at the beginning of Taekwondo. Arthroscopic treatment in symptomatic Taekwondo players is an effective procedure that can improve the postoperative exercise frequency and function. Returning-to-play Taekwondo is associated with the clinical improvements and the patients' will.
MeSH Terms
Figure
-

Figure 1 (A) A frog leg lateral radiograph of a 18-year-old woman professional Taekwondo player, shows a secondary change (black arrow) of the right femoral head-neck junction by pincer impingement. (B) An oblique axial image of CT shows a bump (black arrow) on the right femoral head-neck junction. (C) 3D-CT image. (D) Arthroscopic finding: A debonding unstable acetabular cartilage with labral tear. (E) We performed labral refixation after acetabuloplasty. (F) Arthroscopic femoroplasty was performed.
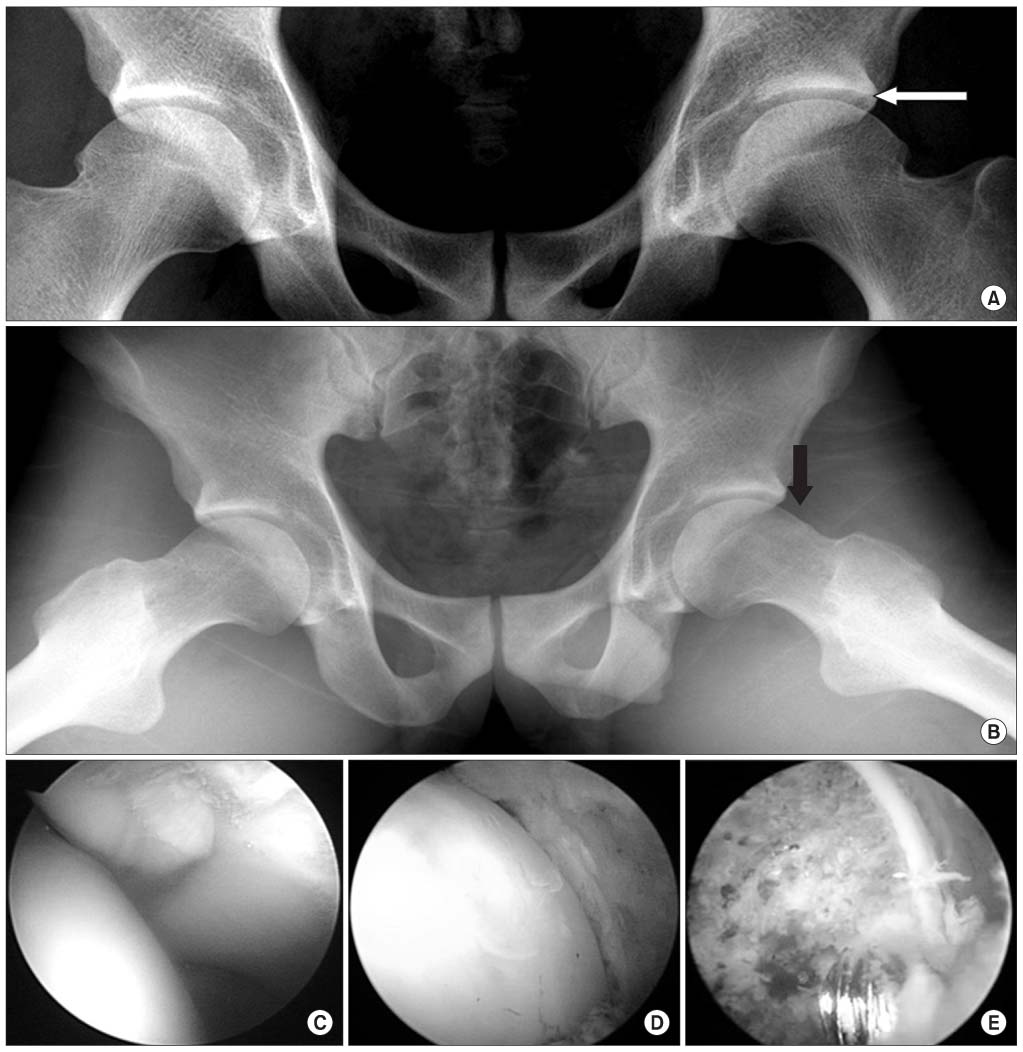
Figure 2 (A) A plain hip AP radiograph of a 22-year-old man, who was a professional Taekwondo player, shows acetabular retroversion (white arrow) on left hip. (B) Plain hip frog leg lateral radiograph shows a finding of decreased femoral offset and femoral flattening (black arrow). (C) Arthroscopic finding: A labrum at 3 o'clock was torn. (D) Acetabuloplasty after partial labrectomy was performed. (E) Femoroplasty was performed.
Cited by 2 articles
-
Paralabral Cysts and Their Correlation with Acetabular Disorder
Chan Kang, Deuk-Soo Hwang, Yoo-Sun Jeon, Dong-Hun Kang, Jae-Whang Song
Hip Pelvis. 2012;24(3):231-236. doi: 10.5371/hp.2012.24.3.231.Femoroacetabular Impingement Syndrome
Chul-Ho Kim, Jae-In Park, Young Hyun Choi, Pil Whan Yoon
J Korean Orthop Assoc. 2017;52(6):467-475. doi: 10.4055/jkoa.2017.52.6.467.
Reference
-
1. Ekström H, Elmståhl S. Pain and fractures are independently related to lower walking speed and grip strength: results from the population study "Good Ageing in Skåne". Acta Orthop. 2006. 77:902–911.
Article2. Altenberg AR. Acetabular labrum tears: a cause of hip pain and degenerative arthritis. South Med J. 1977. 70:174–175.3. Anderson K, Strickland SM, Warren R. Hip and groin injuries in athletes. Am J Sports Med. 2001. 29:521–533.
Article4. Philippon MJ, Schenker ML. Arthroscopy for the treatment of femoroacetabular impingement in the athlete. Clin Sports Med. 2006. 25:299–308.
Article5. Bizzini M, Notzli HP, Maffiuletti NA. Femoroacetabular impingement in professional ice hockey players: a case series of 5 athletes after open surgical decompression of the hip. Am J Sports Med. 2007. 35:1955–1959.6. Brunner A, Horisberger M, Herzog RF. Sports and recreation activity of patients with femoroacetabular impingement before and after arthroscopic osteoplasty. Am J Sports Med. 2009. 37:917–922.
Article7. Laude F, Boyer T, Nogier A. Anterior femoroacetabular impingement. Joint Bone Spine. 2007. 74:127–132.
Article8. Kang C, Hwang DS, Cha SM. Acetabular labral tears in patients with sports injury. Clin Orthop Surg. 2009. 1:230–235.
Article9. Klaue K, Durnin CW, Ganz R. The acetabular rim syndrome. A clinical presentation of dysplasia of the hip. J Bone Joint Surg Br. 1991. 73:423–429.
Article10. Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005. 87:1012–1018.11. Tönnis D. Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop Relat Res. 1976. (119):39–47.12. Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg Br. 2002. 84:556–560.
Article13. Tannast M, Siebenrock KA. Conventional radiographs to assess femoroacetabular impingement. Instr Course Lect. 2009. 58:203–212.14. Reynolds D, Lucas J, Klaue K. Retroversion of the acetabulum. A cause of hip pain. J Bone Joint Surg Br. 1999. 81:281–288.15. Wiberg G. Studies on dysplastic acetabula and congenital subluxation of the hip joint with special reference to the complication of osteo-arthritis. Acta Chir Scand. 1939. Suppl 58. 1–135.16. Tannast M, Siebenrock KA, Anderson SE. Femoroacetabular impingement: radiographic diagnosis--what the radiologist should know. AJR Am J Roentgenol. 2007. 188:1540–1552.
Article17. Beck M, Leunig M, Parvizi J, Boutier V, Wyss D, Ganz R. Anterior femoroacetabular impingement: part II. Midterm results of surgical treatment. Clin Orthop Relat Res. 2004. (418):67–73.18. Glick JM, Sampson TG, Gordon RB, Behr JT, Schmidt E. Hip arthroscopy by the lateral approach. Arthroscopy. 1987. 3:4–12.
Article19. Ide T, Akamatsu N, Nakajima I. Arthroscopic surgery of the hip joint. Arthroscopy. 1991. 7:204–211.
Article20. Philippon M, Schenker M, Briggs K, Kuppersmith D. Femoroacetabular impingement in 45 professional athletes: associated pathologies and return to sport following arthroscopic decompression. Knee Surg Sports Traumatol Arthrosc. 2007. 15:908–914.
Article21. Valderrabano V, Pagenstert G, Horisberger M, Knupp M, Hintermann B. Sports and recreation activity of ankle arthritis patients before and after total ankle replacement. Am J Sports Med. 2006. 34:993–999.
Article22. Christensen CP, Althausen PL, Mittleman MA, Lee JA, McCarthy JC. The nonarthritic hip score: reliable and validated. Clin Orthop Relat Res. 2003. (406):75–83.
Article23. McCarthy J, Barsoum W, Puri L, Lee JA, Murphy S, Cooke P. The role of hip arthroscopy in the elite athlete. Clin Orthop Relat Res. 2003. (406):71–74.
Article24. Wenger DE, Kendell KR, Miner MR, Trousdale RT. Acetabular labral tears rarely occur in the absence of bony abnormalities. Clin Orthop Relat Res. 2004. (426):145–150.
Article25. McCarthy JC, Noble PC, Schuck MR, Wright J, Lee J. The Otto E. Aufranc Award: The role of labral lesions to development of early degenerative hip disease. Clin Orthop Relat Res. 2001. (393):25–37.26. Philippon MJ. The role of arthroscopic thermal capsulorrhaphy in the hip. Clin Sports Med. 2001. 20:817–829.
Article27. Byrd JW, Jones KS. Hip arthroscopy in athletes. Clin Sports Med. 2001. 20:749–761.28. Philippon MJ, Schenker ML, Briggs KK, Kuppersmith DA, Maxwell RB, Stubbs AJ. Revision hip arthroscopy. Am J Sports Med. 2007. 35:1918–1921.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Descriptive Epidemiology of Symptomatic Femoroacetabular Impingement in Young Athlete: Single Center Study
- Controversial Issues in Arthroscopic Surgery for Femoroacetabular Impingement
- Successful Treatment of Anterior Knee Impingement Syndrome in Taekwondo Athletes
- Acetabular Labral Tears in Patients with Sports Injury
- Femoroacetabular Impingement Syndrome
