Common Benign Bone Tumors in Clinic
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul National University College of Medicine, Seoul, Korea. mdchs111@snu.ac.kr
- KMID: 2185154
- DOI: http://doi.org/10.4055/jkoa.2014.49.6.411
Abstract
- Benign bone tumors can be found in the following clinical situations: 1) incidental findings on chest radiograph for health screening without symptoms or radiographs after traffic accident; 2) radiographs for other orthopedic problems, such as osteoarthritis; and 3) pain caused by the tumor. Knowledge of various diseases and their clinical characteristics is required for diagnosis of benign bone tumors. In addition, one should consider carefully whether or not the lesion has the characteristics of benign bone tumor or possibility of malignancy so that proper treatment can be decided. In case the diagnosis cannot be confirmed, even though benign bone tumor is suspected on radiography, follow-up radiographs should be taken to rule-out malignant bone tumors.
Keyword
MeSH Terms
Figure
-

Figure 1 (A) A pedunculated osteochondroma in the distal femur. (B) Antero-posterior radiograph of the knees in a woman with multiple hereditary osteochondromas.

Figure 2 Antero-posterior radiograph of the pelvis in a 22-year-old man with a secondary chondrosarcoma in the pubic bone showing disorganized and irregular calcifications.

Figure 3 Serial radiographs of a 24-year-old man with a secondary chondrosarcoma originating from the proximal tibia (A) radiographs from when the man was 20-year-old (B) radiographs from when he was 24-year-old showing dispersed calcifications within the cartilage cap that are separate from the stalk (black arrows) and erosion of the fibula (white arrow). (C) An axial magnetic resonance image showing a thick cartilage cap and the eroded fibula (white arrow).
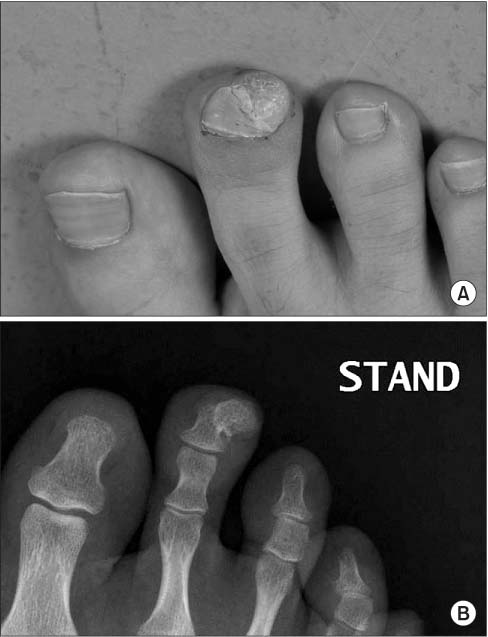
Figure 4 Subungual exostosis originating from the distal phalanx of the second toe.

Figure 5 An enchondroma in the proximal phalanx.

Figure 6 Non-ossifying fibroma of the proximal humerus.

Figure 7 Serial radiographs of a man with a non-ossifiying fibroma in the proximal tibia showing spontaneous regression.

Figure 8 A cortical desmoid in the left distal femur.
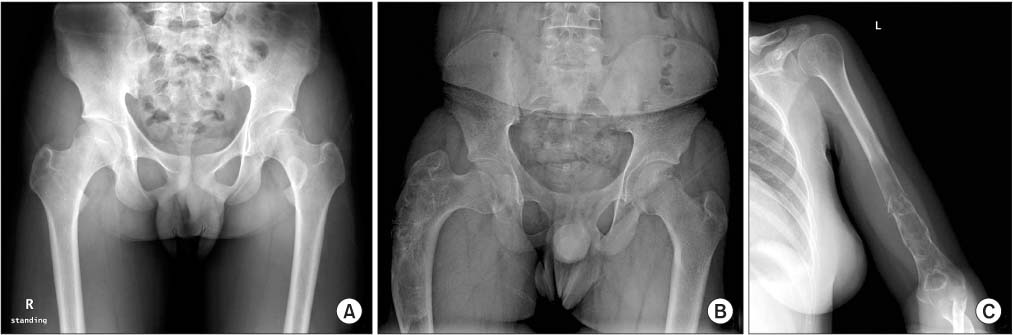
Figure 9 (A) A monostotic fibrous dysplasia in the proximal femur showing a ground glass appearance. (B) A shepherd crook deformity. (C) A pathologic fracture of the humerus in a fibrous dysplasia.

Figure 10 (A) A pathologic fracture through a unicameral bone cyst showing a fallen leaf sign (arrow). (B) Healing of a pathologic fracture accompanied by spontaneous consolidation of a unicameral bone cyst.

Figure 11 Consolidation of a unicameral bone cyst after demineralized bone matrix injection in the lesion.

Figure 12 An osteoid osteoma in the diaphysis of the tibia showing the extensive periosteal reaction and central radiolucency.

Figure 13 (A) An osteoid osteoma in the proximal humerus showing lack of sclerosis around the lesion (arrow). An axial computed tomography image (B) and magnetic resonance image of an osteoid osteoma showing extensive edema around the lesion (C).

Figure 14 Schematic representation of the shave down procedure.

Figure 15 (A) A chondroblastoma in the proximal tibial epiphysis. Radiographs of a chondroblastoma with a pathologic fracture (arrow) (B) in the patella showing an aneurysmal cystic change on magnetic resonance imaging (C).
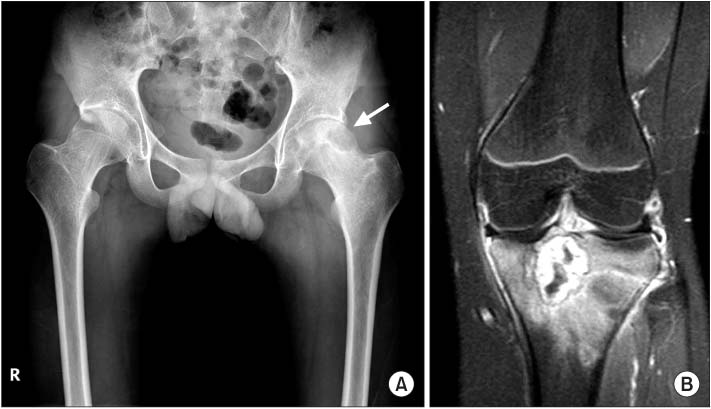
Figure 16 (A) A chondroblastoma in the proximal femoral epiphysis of a 14-year-old boy presenting with limping and limitation of motion in the ipsilateral hip joint (arrow). (B) A coronal magnetic resonance image of a chondroblastoma showing extensive edema around the lesion.

Figure 17 A giant cell tumor in the proximal tibia of a 28-year-old woman.

Figure 18 A giant cell tumor in the distal femur of a 22-year-old man showing a cortical breakage (arrow).

Figure 19 An osteosarcoma in the distal femur mimicking a giant cell tumor.

Figure 20 (A) Langerhans cell histiocytosis involving the skull. (B) A plain radiograph of Langerhans cell histiocytosis in the distal humerus of a 15-year-old boy. (C) Vertebra plana.
Reference
-
1. Garrison RC, Unni KK, McLeod RA, Pritchard DJ, Dahlin DC. Chondrosarcoma arising in osteochondroma. Cancer. 1982; 49:1890–1897.
Article2. Ahmed AR, Tan TS, Unni KK, Collins MS, Wenger DE, Sim FH. Secondary chondrosarcoma in osteochondroma: report of 107 patients. Clin Orthop Relat Res. 2003; 411:193–206.
Article3. Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: variants and complications with radiologic-pathologic correlation. Radiographics. 2000; 20:1407–1434.
Article4. Eliezri YD, Taylor SC. Subungual osteochondroma. Diagnosis and management. J Dermatol Surg Oncol. 1992; 18:753–758.
Article5. Glockenberg A, Sobel E, Noël JF. Nonossifying fibroma. Four cases and review of the literature. J Am Podiatr Med Assoc. 1997; 87:66–69.
Article6. Sposto MR, Navarro CM, de Oliveira MR, Gabrielli MF, Ferreira BA. Albright's syndrome: review of the literature and case report. J Nihon Univ Sch Dent. 1994; 36:283–287.
Article7. Cohen J. Simple bone cysts. Studies of cyst fluid in six cases with a theory of pathogenesis. J Bone Joint Surg Am. 1960; 42:609–616.8. Struhl S, Edelson C, Pritzker H, Seimon LP, Dorfman HD. Solitary (unicameral) bone cyst. The fallen fragment sign revisited. Skeletal Radiol. 1989; 18:261–265.9. Baig R, Eady JL. Unicameral (simple) bone cysts. South Med J. 2006; 99:966–976.
Article10. Kransdorf MJ, Stull MA, Gilkey FW, Moser RP Jr. Osteoid osteoma. Radiographics. 1991; 11:671–696.
Article11. Feletar M, Hall S. Osteoid osteoma: a case for conservative management. Rheumatology (Oxford). 2002; 41:585–586.
Article12. Peyser A, Applbaum Y, Khoury A, Liebergall M, Atesok K. Osteoid osteoma: CT-guided radiofrequency ablation using a water-cooled probe. Ann Surg Oncol. 2007; 14:591–596.
Article13. Martel Villagrán J, Bueno Horcajadas A, Ortiz Cruz EJ. Percutaneous radiofrequency ablation of benign bone tumors: osteoid osteoma, osteoblastoma, and chondroblastoma. Radiologia. 2009; 51:549–558.14. Greenspan A, Steiner G, Knutzon R. Bone island (enostosis): clinical significance and radiologic and pathologic correlations. Skeletal Radiol. 1991; 20:85–90.
Article15. Kyriakos M, Land VJ, Penning HL, Parker SG. Metastatic chondroblastoma. Report of a fatal case with a review of the literature on atypical, aggressive, and malignant chondroblastoma. Cancer. 1985; 55:1770–1789.
Article16. Riddell RJ, Louis CJ, Bromberger NA. Pulmonary metastases from chondroblastoma of the tibia. Report of a case. J Bone Joint Surg Br. 1973; 55:848–853.17. Thomas DM, Skubitz KM. Giant cell tumour of bone. Curr Opin Oncol. 2009; 21:338–344.
Article18. Kirchen ME, Menendez LR, Lee JH, Marshall GJ. Methotrexate eluted from bone cement: effect on giant cell tumor of bone in vitro. Clin Orthop Relat Res. 1996; 328:294–303.19. Bini SA, Gill K, Johnston JO. Giant cell tumor of bone. Curettage and cement reconstruction. Clin Orthop Relat Res. 1995; 321:245–250.20. Chang SS, Suratwala SJ, Jung KM, et al. Bisphosphonates may reduce recurrence in giant cell tumor by inducing apoptosis. Clin Orthop Relat Res. 2004; 426:103–109.
Article21. Thomas DM. RANKL, denosumab, and giant cell tumor of bone. Curr Opin Oncol. 2012; 24:397–403.
Article22. Leikin SL. Immunobiology of histiocytosis-X. Hematol Oncol Clin North Am. 1987; 1:49–61.
Article23. Yasko AW, Fanning CV, Ayala AG, Carrasco CH, Murray JA. Percutaneous techniques for the diagnosis and treatment of localized Langerhans-cell histiocytosis (eosinophilic granuloma of bone). J Bone Joint Surg Am. 1998; 80:219–228.
Article
