Change of Kyphotic Angle in Posterior Pedicle Screw Fixation for Thoracic and Lumbar Burst Fractures: Comparison Study by the Screw Fixation Level
- Affiliations
-
- 1Department of Orthopedic Surgery, Seoul Paik Hospical, College of Medicine, Inje University, Seoul, Korea. hd1404@hanafos.com
- KMID: 2183886
- DOI: http://doi.org/10.12671/jkfs.2009.22.1.39
Abstract
- PURPOSE
To evaluate the relationship between the level of screw fixation and the stability of the segment of endplate fracture after posterior pedicle screw instrumentation for thoracic and lumbar burst fractures.
MATERIALS AND METHODS
The 41 patients of burst fractures who had been operated with pedicle screw instrumentation were retrospectively evaluated. The patients were divided into two groups by the levels of screw fixation. One group was treated with screws fixed by one-level to the direction of fractured endplate (One-level group, 16 cases). The other group was treated with screws fixed by two-level to the direction of endplate fracture (Two-level group, 25 cases). The two groups were compared by the radiographic changes of kyphotic angle between the day of surgery and 6 months after surgery.
RESULTS
At the 6 months, one-level group showed the change of kyphotic angle of 17.5+/-2.4 degrees, which was different from two-level group of 5.2+/-0.8 degrees (p=0.000).
CONCLUSION
In posterior pedicle screws fixation for thoracic and lumbar burst fractures, 2 vertebrae to the direction of the endplate fracture should be included to prevent the postoperative kyphotic change.
Keyword
MeSH Terms
Figure
-

Fig. 1 Denis classification. Asterisk (*) indicates unstable segment.
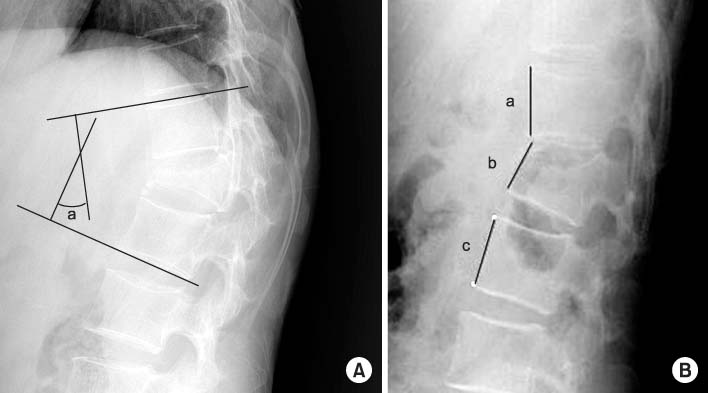
Fig. 2 Measurement methods of kyphotic angle and vertebral body height. (A) Kyphotic angle (a) measured by the Cobbs' method. (B) Anterior vertebral height loss (%) measured by {1-b/(a+c/2)}×100.
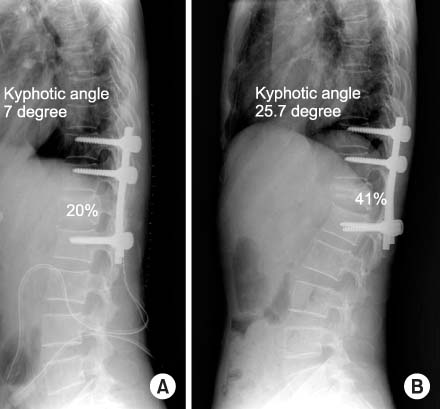
Fig. 3 A 47 year old woman sustained Denis type A burst fracture of L1. (A) Immediately postoperative lateral view shows 7 degree of kyphotic angle and 20% of anterior vertebral height loss. (B) Postoperative 6 months lateral view shows unstable fixation of 25.7 degree of kyphotic angle and 41% of anterior vertebral height loss.
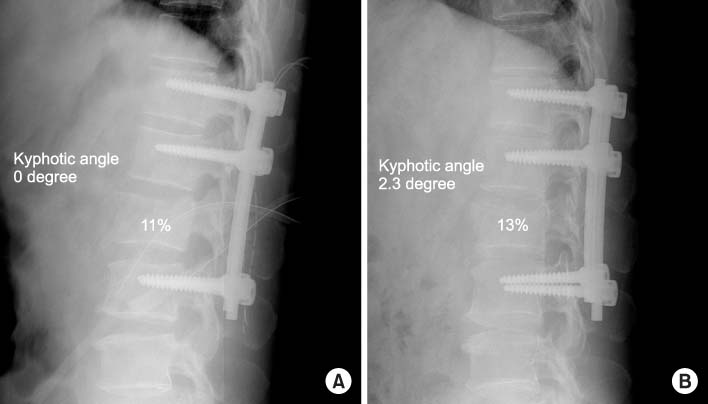
Fig. 4 A 54 year old man sustained Denis type B burst fracture of L2. (A) Immediately postoperative lateral view shows 0 degree of kyphotic angle and 11% of anterior vertebral height loss. (B) Postoperative 6 months lateral view shows stable fixation of 2.3 degree of kyphotic angle and 13% of anterior vertebral height loss.
Reference
-
1. Carl AL, Tromanhauser SG, Roger DJ. Pedicle screw instrumentation for thoracolumbar burst fractures and fracture-dislocations. Spine (Phila Pa 1976). 1992; 17:Suppl 8. S317–S324.
Article2. Cho JL, Park YS, Kim DH. Operative treatment of burst fracture in thoracolumbar and lumbar spine using Kaneda instrument. J Korean Soc Spine Surg. 1997; 4:81–89.3. Danisa OA, Shaffrey CI, Jane JA, et al. Surgical approaches for the correction of unstable thoracolumbar burst fractures: a retrospective analysis of treatment outcomes. J Neurosurg. 1995; 83:977–983.
Article4. Denis F. The three column spine and its significance in the classification of acute thoracolumbar spinal injuries. Spine. 1983; 8:817–831.
Article5. Denis F. Spinal instability as defined by three-column spine concept in acute spinal trauma. Clin Orthop Relat Res. 1984; 189:65–76.6. Dickson JH, Harrington PR, Erwin WD. Results of reduction and stabilization of the severely fractured thoracic and lumbar spine. J Bone Joint Surg Am. 1978; 60:799–805.
Article7. Daniaux H, Seykora P, Genelin A, Lang T, Kathrein A. Application of posterior plating and modifications in thoracolumbar spine injuries. Indication, techniques, and results. Spine (Phila Pa 1976). 1991; 16:3 Suppl. S125–S133.8. Esses SI, Botsford DJ, Kostuik JP. Evaluation of surgical treatment for burst fractures. Spine. 1990; 15:667–673.
Article9. Gaines RW Jr. The use of pedicle-screw internal fixation for the operative treatment of spinal disorders. J Bone Joint Surg Am. 2000; 82:1458–1476.
Article10. Gertzbein SD, Court-Brown CM, Jacobs RR, et al. Decompression and circumferential stabilization of unstable spinal fractures. Spine. 1988; 13:892–895.
Article11. Grob D, Scheier HJ, Dvorak J, Siegrist H, Rubeli M, Joller R. Circumferential fusion of the lumbar and lumbosacral spine. Arch Orthop Trauma Surg. 1991; 111:20–25.
Article12. Hahn KH, Lee SG, Jeong JH, Yoo CJ, Kim WK, Kim YB. One stage decompression and circumferential stabilization by posterior approach in the unstable burst fracture of thoracolumbar and lumbar spine. J Korean Neurosurg Soc. 2002; 32:112–117.13. Ahn JS, Lee JK, Hwang DS, Kim YM, Kim WJ, Byun KH. The change of kyphotic angle and anterior vertebral height after posterior or posterolateral fusion with transpedicular screws for thoracolumbar bursting fractures. J Korean Soc Fract. 1999; 12:379–387.
Article14. Jeong ST, Cho SH, Song HR, Koo KH, Park HB, Chung UH. Comparison of short and long segment fusion in thoracic and lumbar fractures. J Korean Soc Spine Surg. 1999; 6:73–80.15. Kim CH, Hwang JK, Choi YJ, Kim KH, Song JS, Kang JH. Treatment of thoraco-lumbar bursting fractures according to load-sharing classification. J Korean Fract Soc. 2005; 18:69–75.
Article16. Kim SK, Byun YS, Lee SW. Surgical treatment of thoracolumbar fractures with transpedicular screws. J Korean Orthop Assoc. 1993; 28:607–615.
Article17. Lee KY, Sohn SK, Kim CH, Song CK. Posterior short-segment instrumentation of thoracic and lumbar bursting fractures: retrospective study related with load-sharing classification. J Korean Soc Spine Surg. 2001; 8:497–503.
Article18. McAfee PC, Bohlman HH, Yuan HA. Anterior decompression of traumatic thoracolumbar fractures with incomplete neurological deficit using a retroperitoneal approach. J Bone Joint Surg Am. 1985; 67:89–104.
Article19. McAfee PC, Yuan HA, Lasda NA. The unstable burst fracture. Spine. 1982; 7:365–373.
Article20. McLain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg Am. 1993; 75:162–167.
Article21. Muller U, Berlemann U, Sledge J, Schwarzenbach O. Treatment of thoracolumbar burst fractures without neurologic deficit by indirect reduction posterior instrumentation: bisegmental stabilization with monosegmental fusion. Eur Spine J. 1999; 8:284–289.22. Ohlin A, Karlsson M, Duppe H, Hasserius R, Redlund-Johnell I. Complication after transpedicular stabilization of the spine. A survivorship analysis of 163 cases. Spine. 1994; 19:2774–2779.
Article23. Park HJ, Lee DH, Lim MH. The effectiveness of transpedicular bone graft in burst fracture. J Korean Soc Spine Surg. 2000; 7:625–631.24. Parker JW, Lane JR, Karaikovic EE, Gaines RW. Successful short-segment instrumentation and fusion for thoracolumbar spine fractures: a consecutive 41/2-year series. Spine. 2000; 25:1157–1170.
Article25. Park YS, Kim YS, Kang CN, Choi CH, Cho JL. Comparative analysis of unstable burst fracture according to the methodology of surgical treatment. J Korean Soc Spine Surg. 2004; 11:278–284.
Article26. Shin BJ, Kim BW, Lee S. The effect of anterior column augmentation in thoraco - lumbar burst fractures treated with pedicle screw instrumentation. J Korean Soc Spine Surg. 1997; 4:223–231.27. Song KJ, Lee KR, Jeon JY. Surgical treatment for the thoracolumbar burst fractures with neurologic deficit. -a comparative study between anterior and posterior approach-. J Korean Orthop Assoc. 2000; 35:154–160.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Short- and Long-segment Pedicle Screw Fixation with Anterior Interbody Fusion with Short Bone Graft in Denis type B Burst Fractures
- The Effect of Anterior Column Augmentation in Thoraco-lumbar Burst Fractures Treated with Pedicle Screw Instrumentation
- Decision of Posterior Fixation Level by Load-Sharing Classification in Thoracolumbar and Lumbar Burst Fracture
- Significance of Anterior Support in Thoracolumbar Burst Fracture: Single Stage Interbody Fusion with Transpedicular Screw Fixation Versus Pedicle Screw Fixation with Lamina Onlay Fusion
- One Stage Decompression and Circumferential Stabilization by Posterior Approach in the Unstable Burst Fracture of Thoracolumbar and Lumbar Spine
