J Korean Foot Ankle Soc.
2014 Jun;18(2):62-67. 10.14193/jkfas.2014.18.2.62.
Analysis of Clinical and Radiographic Outcome of the Reconstructive Surgery for the Cavovarus Foot Deformity
- Affiliations
-
- 1Department of Orthopedic Surgery, Konkuk University School of Medicine, Seoul, Korea. eoms1234@naver.com
- 2Department of Orthopedic Surgery, Hallym University Sacred Heart Hospital, Anyang, Korea.
- KMID: 2181662
- DOI: http://doi.org/10.14193/jkfas.2014.18.2.62
Abstract
- PURPOSE
Reconstructive surgeries for equinocavovarus foot deformities are quite variable, including hind-midfoot osteotomy or arthrodesis, soft tissue procedure, tendon transfers, etc. Comprehensive evaluation of the deformity and its etiology is mandatory for achievement of successful deformity correction. Few studies in this field have been reported. We report on the clinical and radiographic outcome of reconstruction for cavovarus foot deformities.
MATERIALS AND METHODS
The study is based on 16 feet with cavovarus foot deformities that underwent bony and soft tissue reconstructive surgery from 2004 to 2008. We evaluated the etiologies, varieties of surgical procedures performed, pain score, functional scores, and patient satisfaction and measured the radiographic parameters.
RESULTS
The average age at the time of surgery was 39.4 years old, with a male/female ratio of 9/4 and an average follow-up period of 23.9 months (range, 12~49 months). The etiologies of the cavovarus deformity were idiopathic 7 feet, residual poliomyelitis 5 feet, Charcot-Marie-Tooth disease 2 feet, and Guillain-Barre syndrome and hemiplegia due to cerebrovascular accident sequela 1 foot each. Lateral sliding calcaneal osteotomies were performed in 12 feet (75%), followed by Achilles tendon lengthening and plantar fascia release in 11 feet (69%), and first metatarsal dorsiflexion osteotomy/arthrodesis and tendon transfer in 10 feet (63%). Visual analogue scale pain score showed improvement, from an average of 4.2 to 0.5 points. American Orthopaedic Foot and Ankle Society ankle-hindfoot score showed significant improvement, from 47.8 to 90.0 points (p<0.05). All patients were satisfied. Ankle range of motion improved from 27.5degrees to 46.7degrees. In radiographic measurements, calcaneal pitch angle improved from 19.1degrees to 15.8degrees, Meary angle from 13.0degrees to 9.3degrees, Hibb's angle from 44.3degrees to 37.0degrees, and tibio-calcaneal axis angle from varus 17.5degrees to varus 1.5degrees.
CONCLUSION
We achieved successful correction of cavovarus foot deformities by performing appropriate comprehensive reconstructive procedures with improved functional, radiographic measures and high patient satisfaction.
Keyword
MeSH Terms
Figure
-
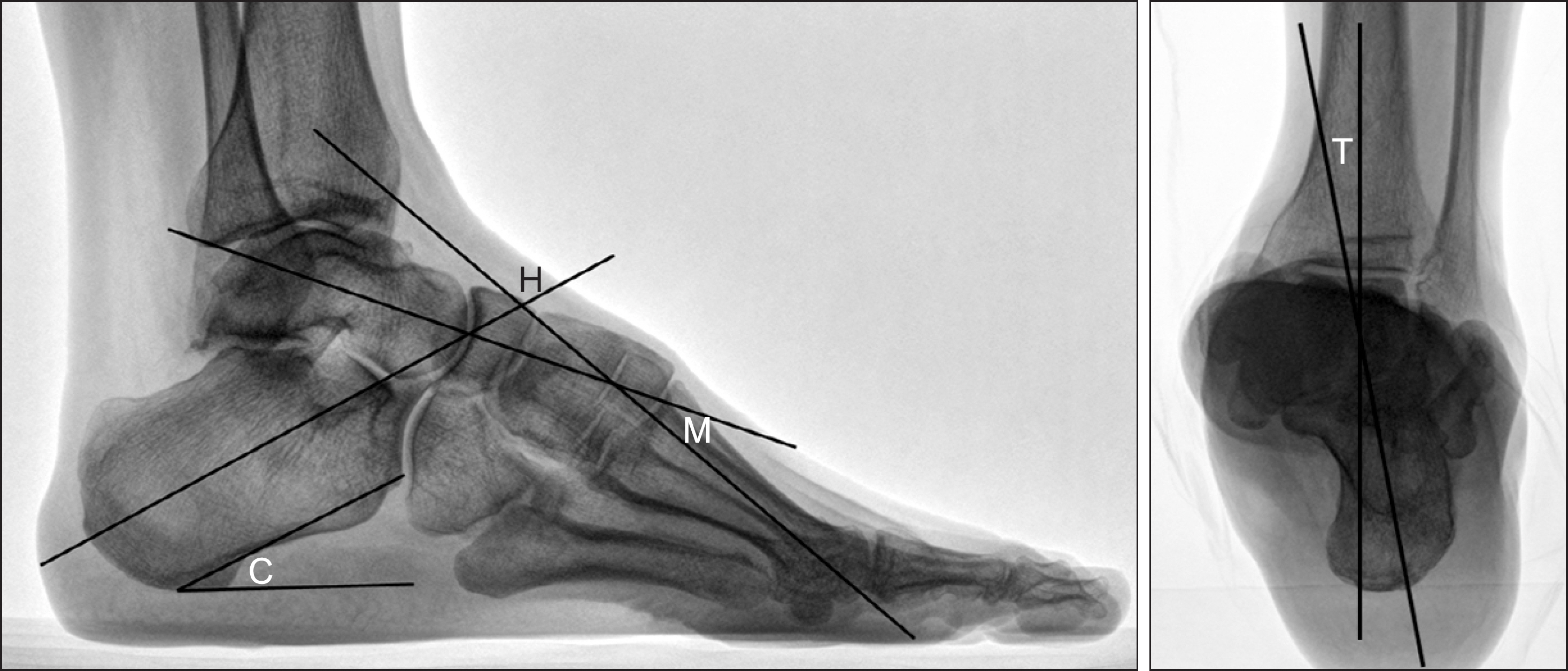
Figure 1. Plain weight bearing lateral radiograph shows the Meary angle (M), Hibb's angle (H), calcaneal pitch angle (C), and tibio-calcaneal axis angle (T).

Figure 2. Plain weight bearing lateral radiographs of a 34-year-old female with idiopathic cavovarus foot; preoperative (A) and postoperative (B).
Reference
-
References
1. Ortiz C, Wagner E, Keller A. Cavovarus foot reconstruction. Foot Ankle Clin. 2009; 14:471–87.
Article2. Giannini S, Ceccarelli F, Benedetti MG, Faldini C, Grandi G. Surgical treatment of adult idiopathic cavus foot with plantar fasciotomy, naviculocuneiform arthrodesis, and cuboid osteotomy. A review of thirty-nine cases. J Bone Joint Surg Am. 2002; 84(Suppl 2):62–9.3. Sammarco GJ, Taylor R. Cavovarus foot treated with combined calcaneus and metatarsal osteotomies. Foot Ankle Int. 2001; 22:19–30.
Article4. Wülker N, Hurschler C. Cavus foot correction in adults by dorsal closing wedge osteotomy. Foot Ankle Int. 2002; 23:344–7.
Article5. Chu IT, Park JM, Yoo JM, Chung JW. Combined first metatarsal and calcaneal osteotomy for fixed cavovarus deformity of the foot. J Korean Foot Ankle Soc. 2010; 14:130–4.6. Kitaoka HB, Alexander IJ, Adelaar RS, Nunley JA, Myerson MS, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int. 1994; 15:349–53.
Article7. McCluskey WP, Lovell WW, Cummings RJ. The cavovarus foot deformity. Etiology and management. Clin Orthop Relat Res. 1989; 247:27–37.8. Beals TC, Nickisch F. Charcot-Marie-Tooth disease and the cavovarus foot. Foot Ankle Clin. 2008; 13:259–74.
Article9. Coleman SS, Chesnut WJ. A simple test for hindfoot flexibility in the cavovarus foot. Clin Orthop Relat Res. 1977; 123:60–2.
Article10. Samilson RL, Dillin W. Cavus, cavovarus, and calcaneocavus. An update. Clin Orthop Relat Res. 1983; 177:125–32.11. Dreher T, Hagmann S, Wenz W. Reconstruction of multiplanar deformity of the hindfoot and midfoot with internal fixation techniques. Foot Ankle Clin. 2009; 14:489–531.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Diagnosis and Operation Results for Chronic Lateral Ankle Instability with Subtle Cavovarus Deformity and a Peek-A-Boo Heel Sign
- Combined First Metatarsal and Calcaneal Osteotomy for Fixed Cavovarus Deformity of The Foot
- Predisposing Factors and Treatment for the Fifth Proximal Metatarsal Fracture
- Clinical Utility of Radiographic Measurements of Insertional Achilles Tendinitis with Haglund's Deformity
- Changes in Dynamic Pedobarography after Extensive Plantarmedial Release for Paralytic Pes Cavovarus
