Comparison of Operative Results of Distal Chevron Osteotomy with and without Akin Osteotomy for Moderate to Severe Hallux Valgus
- Affiliations
-
- 1Department of Orthopaedic Surgery, College of Medicine, Chosun University, Gwangju, Korea. leejy88@chosun.ac.kr
- KMID: 2181661
- DOI: http://doi.org/10.14193/jkfas.2014.18.2.56
Abstract
- PURPOSE
This study was conducted among patients with moderate to severe hallux valgus who underwent distal chevron osteotomy and groups of patients with or without Akin osteotomy were compared for evaluation of the relationship between their radiological and clinical outcomes.
MATERIALS AND METHODS
From January 2009 to January 2012, among patients with moderate to severe hallux valgus who underwent distal chevron osteotomy at our institution, 28 cases with additional Akin osteotomy and 35 cases without Akin osteotomy available to follow up of more than one year were included in this study. For radiologic evaluation, hallux valgus angle, 1, 2 intermetatarsal angle, and hallux interphalangeal angle were measured before and after surgery. For clinical assessment, visual analogue scale score, American Orthopaedic Foot and Ankle Society score, subjective satisfaction of the patients, and passive range of motion of the first metatarsophalangeal joints were evaluated.
RESULTS
At the final follow up, correction of valgus hallux angle and 1, 2 intermetatarsal angle was obtained from radiation results of both groups and it was found that patients who underwent Akin osteotomy showed radiographically larger angle correction but less subjective satisfaction.
CONCLUSION
Patients with moderate to severe hallux valgus who underwent distal chevron osteotomy showed not only functional but also radiographically satisfactory results, and patients who underwent additional Akin osteotomy showed decreased subjective satisfaction. Therefore, if an incongruent first metatarsophalangeal joint is not observed, distal chevron osteotomy without Akin osteotomy seems preferable.
MeSH Terms
Figure
-
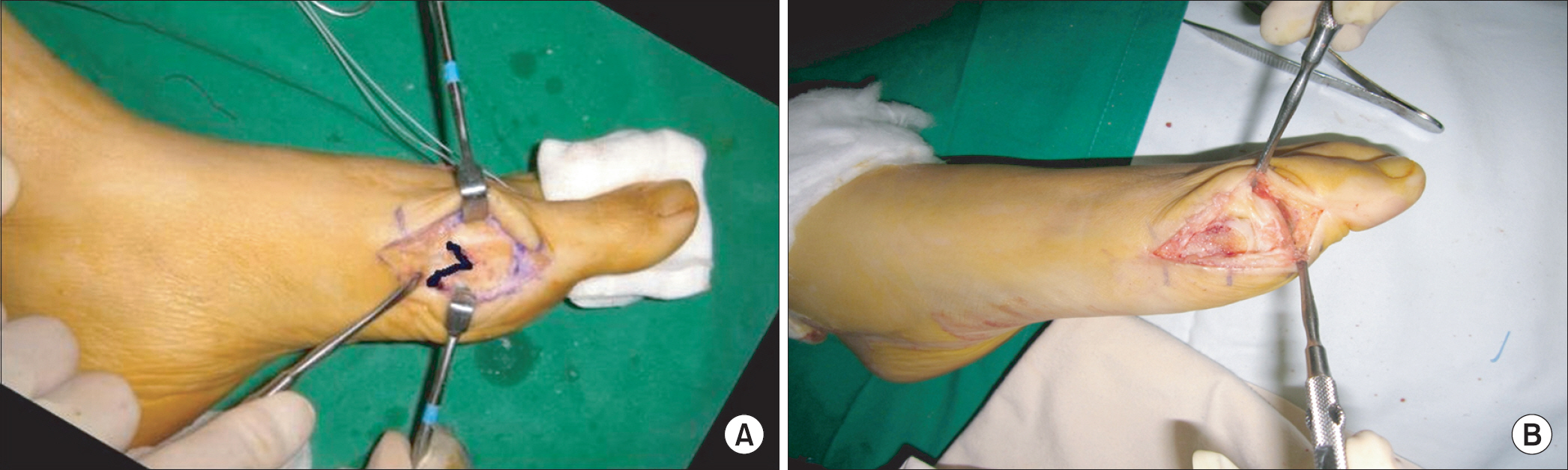
Figure 1. Intraoperative photos show the distal chevron osteotomy (A) and Akin osteotomy (B).

Figure 2. The right foot of 46-year-old female shows moderate hallux valgus deformity. The deformity was corrected with distal chevron metatarsal osteotomy and distal soft tissue procedure. (A) Preoperative hallux valgus angle was 31.2o, the 1st intermetatarsal angle was 18.4o, and the hallux interphalangeal angle was 7.81o. (B) Postoperative hallux valgus angle was 3.4o, the 1st intermetatarsal angle was 8.5o, and the hallux interphalangeal angle was 7.6o. (C) At postoperative 13 months, the hallux valgus angle was 6.3o, the 1st intermetatarsal angle was 8.0o, and the hallux interphalangeal angle was 12.1o. Clinical result was good with no pain and no limitation of activity.
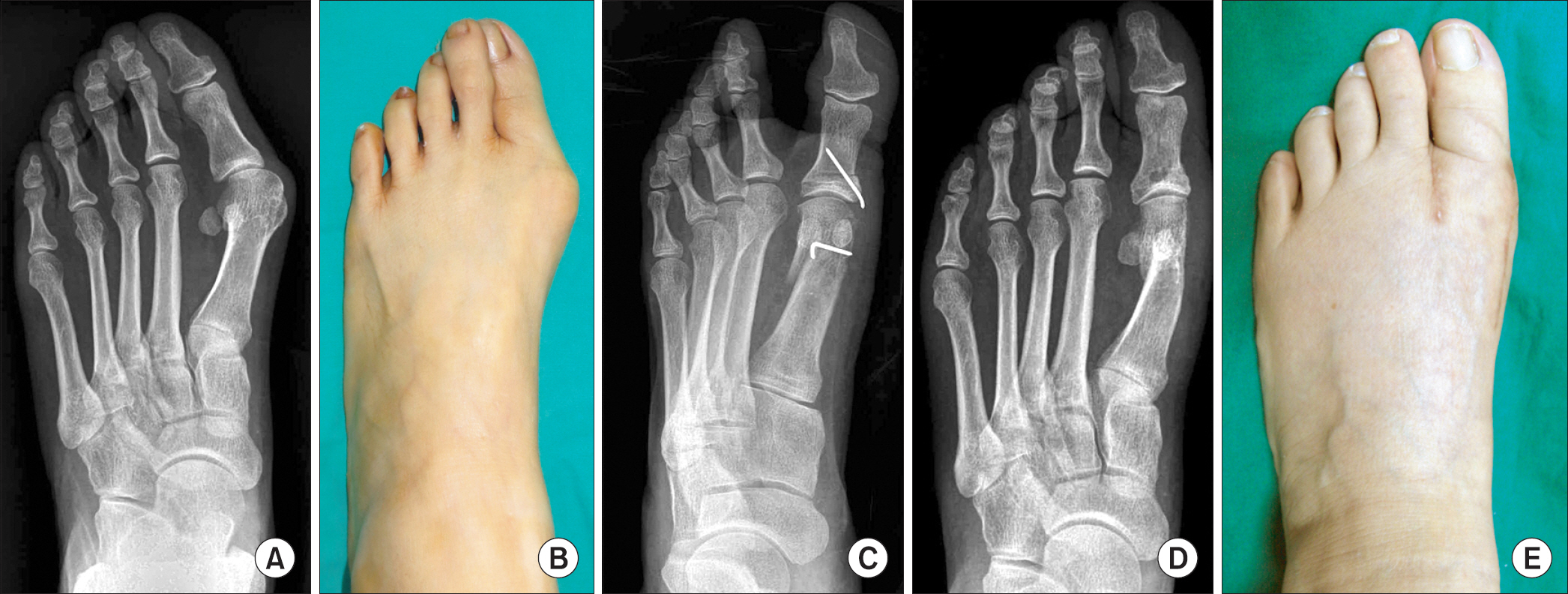
Figure 3. The left foot of 54-year-old female shows severe hallux valgus deformity. The deformity was adequately corrected with distal chevron metatarsal osteotomy, distal soft tissue procedure, and Akin procedure. (A, B) Preoperative hallux valgus angle was 39.2o, the 1st intermetatarsal angle was 11.5o, and the hallux interphalangeal angle was 2.1o. (C) Postoperative hallux valgus angle was 2.0o, the 1st intermetatarsal angle was 6.1o, and the hallux interphalangeal angle was 1.16o. (D, E) At postoperative 12 months, the radiograph and the gross photo show well maintained correction of the deformity. Hallux valgus angle was 10.0o, the 1st intermetatarsal angle was 4.0o, and the hallux interphalangeal angle was 1.9o. Subjective satisfaction was very good although passive range of motion in the 1st metatarsophalangeal joint was moderately restricted.
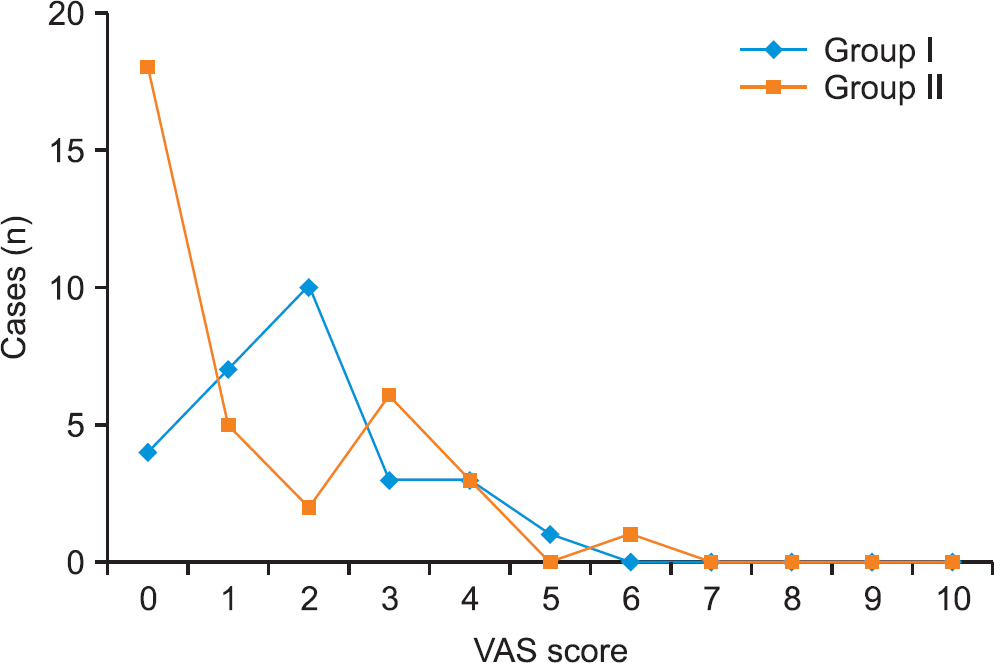
Figure 4. Comparison of visual analogue scale (VAS) score between the isolated distal chevron osteotomy and the distal chevron osteotomy with Akin procedure. Group I: distal chevron metatarsal osteotomy with Akin osteotomy. Group II: isolated distal chevron metatarsal osteotomy.
Cited by 2 articles
-
Comment on“Comparison of Operative Results of Distal Chevron Osteotomy with and without Akin Osteotomy for Moderate to Severe Hallux Valgus”
Jin Su Kim
J Korean Foot Ankle Soc. 2014;18(3):137-137. doi: 10.14193/jkfas.2014.18.3.137.Response to: Comment on“Comparison of Operative Results of Distal Chevron Osteotomy with and without Akin Osteotomy for Moderate to Severe Hallux Valgus”
Sang Soo Park, Jun Young Lee, Woong Hee Kim
J Korean Foot Ankle Soc. 2014;18(3):138-139. doi: 10.14193/jkfas.2014.18.3.138.
Reference
-
References
1. Austin DW, Leventen EO. A new osteotomy for hallux valgus: a horizontally directed "V" displacement osteotomy of the metatarsal head for hallux valgus and primus varus. Clin Orthop Relat Res. 1981; 157:25–30.2. Bai LB, Lee KB, Seo CY, Song EK, Yoon TR. Distal chevron osteotomy with distal soft tissue procedure for moderate to severe hallux valgus deformity. Foot Ankle Int. 2010; 31:683–8.
Article3. Yoo WJ, Chung MS, Baek GH, Yu CH, Moon HJ. Distal chevron osteotomy for moderate to severe hallux valgus deformity in patients aged 50 or older. J Korean Orthop Assoc. 2008; 43:445–50.
Article4. Sanhudo JA. Correction of moderate to severe hallux valgus deformity by a modified chevron shaft osteotomy. Foot Ankle Int. 2006; 27:581–5.
Article5. Silberman FS. Proximal phalangeal osteotomy for the correction of hallux valgus. Clin Orthop Relat Res. 1972; 85:98–100.
Article6. Young KW, Lee KT, Kim JY, Cha SD, Kim ES. Fixation with suture material in akin osteotomy. J Korean Foot Ankle Soc. 2004; 8:138–41.7. Kwon DJ, Song SY, Lee KB, Rhee NK, Choi JH. Results of the ludloff osteotomy for moderate to severe hallux valgus deformity. J Korean Foot Ankle Soc. 2007; 11:166–70.8. Ahn JH, Kim WJ, Kim HY, Choy WS, Kang SI. Treatment of moderate hallux valgus with proximal chevron metatarsal osteotomy and distal soft tissue procedure. J Korean Foot Ankle Soc. 2007; 11:39–44.9. Pinney SJ, Song KR, Chou LB. Surgical treatment of severe hallux valgus: the state of practice among academic foot and ankle surgeons. Foot Ankle Int. 2006; 27:1024–9.
Article10. Lee KT, Choi JH, Young KW, Lee YK, Kim JS, Park JM. Proximal metatarsal chevron osteotomy for moderate to severe hallux valgus: a mean eight year follow up. J Korean Foot Ankle Soc. 2007; 11:154–9.11. Okuda R, Kinoshita M, Yasuda T, Jotoku T, Shima H. Proximal metatarsal osteotomy for hallux valgus: comparison of outcome for moderate and severe deformities. Foot Ankle Int. 2008; 29:664–70.
Article12. Shima H, Okuda R, Yasuda T, Jotoku T, Kitano N, Kinoshita M. Radiographic measurements in patients with hallux valgus before and after proximal crescentic osteotomy. J Bone Joint Surg Am. 2009; 91:1369–76.
Article13. Barouk LS. Forefoot reconstruction. Vol. 3. 2nd ed.Paris, New York: Springer;2005.14. Moon GH, Ahn GY, Lee YH, Nam IH, Lee JI. The effect of derotational closing wedge Akin osteotomy for the treatment of hallux valgus with the pronation of great toe. J Korean Foot Ankle Soc. 2008; 12:14–9.15. Schneider W, Aigner N, Pinggera O, Knahr K. Chevron osteotomy in hallux valgus. Ten-year results of 112 cases. J Bone Joint Surg Br. 2004; 86:1016–20.16. Schneider W, Knahr K. Keller procedure and chevron osteotomy in hallux valgus: five-year results of different surgical philosophies in comparable collectives. Foot Ankle Int. 2002; 23:321–9.
Article17. Colloff B, Weitz EM. Proximal phalangeal osteotomy in hallux valgus. Clin Orthop Relat Res. 1967; 54:105–13.
Article18. Lechler P, Feldmann C, Köck FX, Schaumburger J, Grifka J, Handel M. Clinical outcome after chevron-Akin double osteotomy versus isolated chevron procedure: a prospective matched group analysis. Arch Orthop Trauma Surg. 2012; 132:9–13.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comment on "Comparison of Operative Results of Distal Chevron Osteotomy with and without Akin Osteotomy for Moderate to Severe Hallux Valgus"
- Response to: Comment on "Comparison of Operative Results of Distal Chevron Osteotomy with and without Akin Osteotomy for Moderate to Severe Hallux Valgus"
- Comparison of Proximal Metatarsal Osteotomy andDistal Chevron Osteotomy for Correction of Hallux Valgus
- Comparison of Proximal and Modified Distal Chevron Osteotomy for the Treatment of Moderate to Severe Hallux Valgus Deformity
- Treatment of Severe Hallux Valgus Deformity with Proximal Reverse Chevron Metatarsal Osteotomy and Akin Osteotomy
