Follow-Up of 58 Traumatic Carotid-Cavernous Fistulas after Endovascular Detachable-Balloon Embolization at a Single Center
- Affiliations
-
- 1Department of Radiology, The First Affiliated Hospital of Nanjing Medical University, Nanjing, China. hbshi346@163.com
- KMID: 2179166
- DOI: http://doi.org/10.3988/jcn.2013.9.2.83
Abstract
- BACKGROUND AND PURPOSE
This study evaluated the clinical value of detachable-balloon embolization for traumatic carotid-cavernous fistula (TCCF), focusing on the frequency, risk factors, and retreatment of recurrence.
METHODS
Fifty-eight patients with TCCF underwent transarterial detachable-balloon embolization between October 2004 and March 2011. The clinical follow-up was performed every 3 months until up to 3 years postprocedure. Each patient was placed in either the recurrence group or the nonrecurrence group according to whether a recurrence developed after the first procedure. The relevant factors including gender, fistula location, interval between trauma and the interventional procedure, blood flow in the carotid-cavernous fistula, number of balloons, and whether the internal carotid artery (ICA) was sacrificed were evaluated.
RESULTS
All 58 TCCFs were successfully treated with transarterial balloon embolization, including 7 patients with ICA sacrifice. Recurrent fistulas occurred in seven patients during the follow-up period. Univariate analysis indicated that the interval between trauma and the interventional procedure (p=0.006) might be the main factor related to the recurrence of TCCF. The second treatments involved ICA sacrifice in two patients, fistula embolization with balloons in four patients, and placement of a covered stent in one patient.
CONCLUSIONS
Detachable balloons can still serve as the first-line treatment for TCCFs and recurrent TCCFs despite having a nonnegligible recurrence rate. Shortening the interval between trauma and the interventional procedure may reduce the risk of recurrence.
Keyword
MeSH Terms
Figure
-
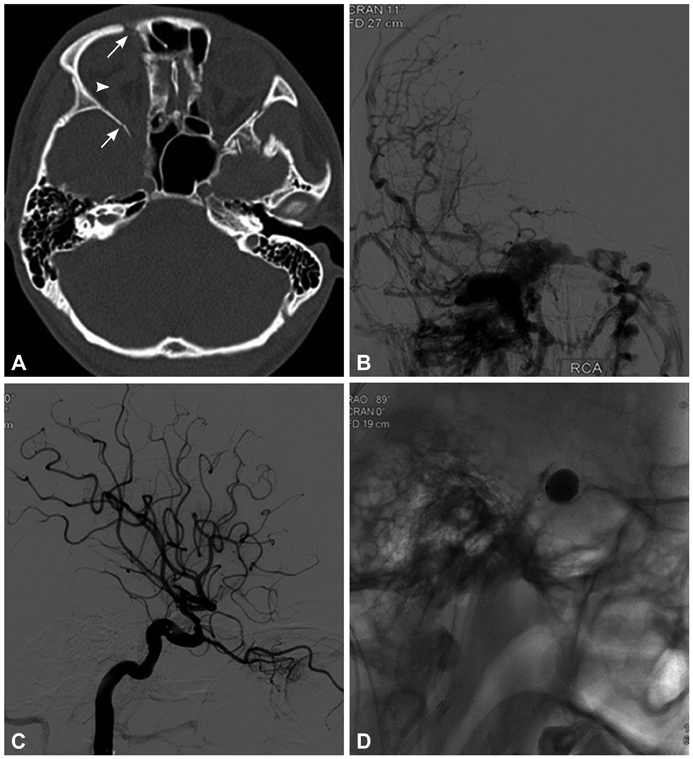
Fig. 1 A 23-year-old man who presented with right-sided proptosis, chemosis, orbital bruit, and decreased visual acuity that occurred 7 days after head blunt trauma. A: Computed tomography indicated right-sided proptosis (arrowhead), superior ophthalmic vein enlargement, and multiple orbital fractures (arrows). B: Cerebral angiography confirmed a high-flow direct carotid-cavernous fistulas that drained into the superior ophthalmic vein, inferior petrosal sinus, intercavernous sinus, and contralateral cavernous sinuses with cortical reflux. C and D: Immediate angiography after single-balloon embolization showed occlusion of the fistula and preservation of the internal carotid artery.
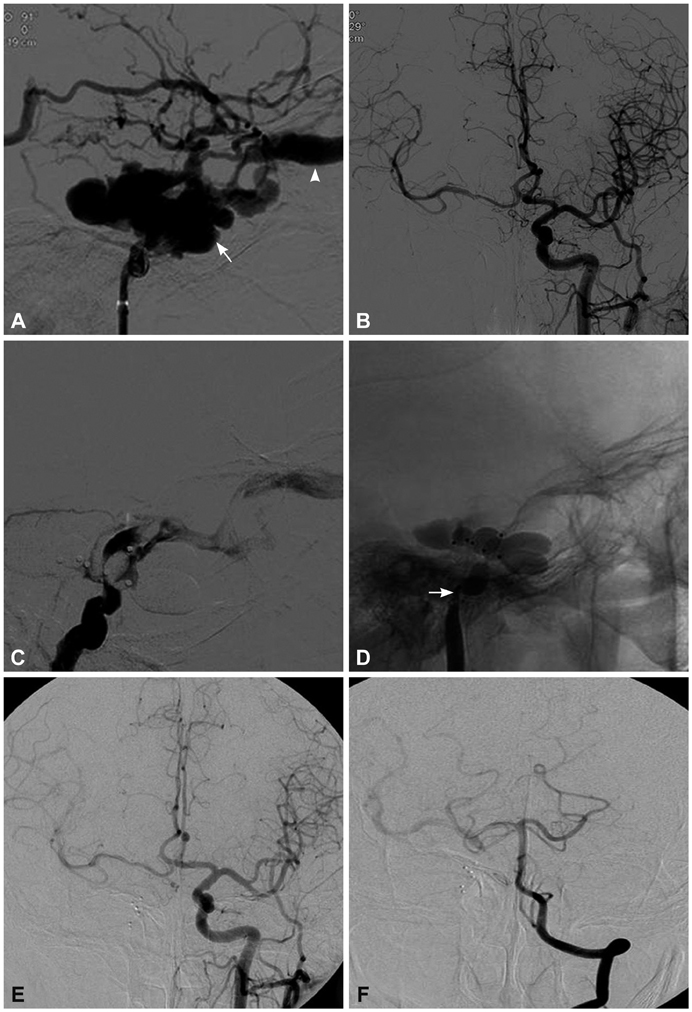
Fig. 2 A 50-year-old man who presented with right-sided chemosis, proptosis, orbital bruit, and lost visual acuity that occurred 61 days after head blunt trauma. A: Lateral cerebral angiography showed a high-flow TCCF that mainly drained into the ophthalmic vein (arrow-head), and (B) contralateral cerebral angiography confirmed good hemodynamic compensation via the communicating artery. C: Angiography showed a residual fistula after embolizations using five balloons, of which two ballons were punctured during the procedure, and hence the ICA was sacrificed (arrow) (D). E and F: Cerebral angiography at the 2-month follow-up showed good compensation via the circle of Willis; the fistula had completely disappeared.
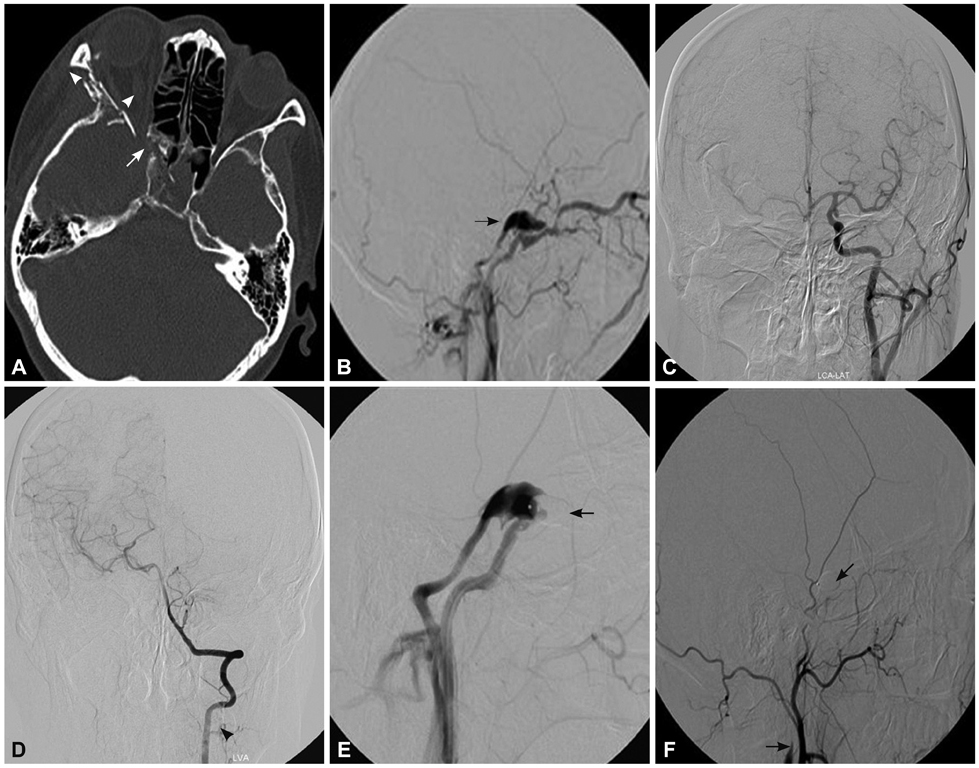
Fig. 3 A 42-year-old woman who presented with right-sided proptosis, chemosis, orbital bruit, and headache 35 days after a vehicle accident. A: Computed tomography indicated right-sided proptosis, superior ophthalmic vein enlargement (arrowhead), and multiple orbital fractures (arrow). B: Cerebral angiography confirmed a high-flow direct CCF that drained into the superior ophthalmic vein and inferior petrosal sinus with cortical reflux (arrow). C and D: Cerebral angiography of the contralateral ICA confirmed good compensation of the circle of Willis. E: Cerebral angiography of the ipsilateral ICA after two-balloon embolization confirmed partial occlusion of the fistula and absence of the distal ICA (arrow), which prompted a diagnosis of obliteration of the ipsilateral ICA distal to the fistula point. F: The CCF was successfully treated after subsequent occlusion of the proximal ICA with a detachable balloon (arrow). CCF: carotid-cavernous fistula, ICA: internal carotid artery.
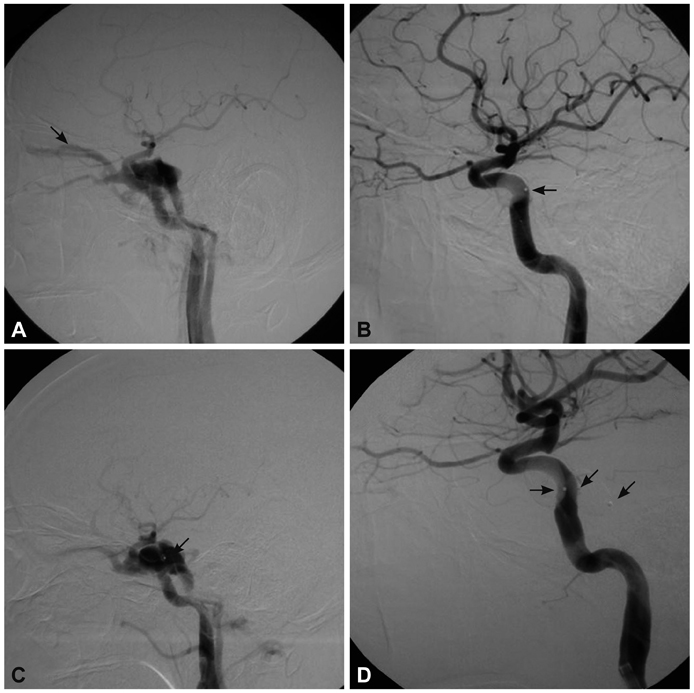
Fig. 4 A 43-year-old man who presented with left-sided proptosis, chemosis, diplopia, and orbital bruit 70 days after a vehicle accident. A: Cerebral angiography confirmed an intermediate-flow direct CCF that drained into the superior ophthalmic vein (arrow). B: Immediate angiography after a single-balloon embolization showed occlusion of the fistula and preservation of the ICA (arrow). C: The patient developed a recurrent fistula on day 7 after the initial embolization, which was attributed to premature deflation and migration of the balloon (arrows) (D). Two detachable balloons were subsequently deployed, which resulted in successful treatment of the RTCCF (arrow). CCF: carotid-cavernous fistula, ICA: internal carotid artery, RTCCF: recurrent traumatic CCF.
Reference
-
1. Barnwell SL, O'Neill OR. Endovascular therapy of carotid cavernous fistulas. Neurosurg Clin N Am. 1994. 5:485–495.
Article2. Barrow DL, Spector RH, Braun IF, Landman JA, Tindall SC, Tindall GT. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985. 62:248–256.
Article3. Serbinenko FA. Balloon catheterization and occlusion of major cerebral vessels. J Neurosurg. 1974. 41:125–145.
Article4. Lewis AI, Tomsick TA, Tew JM Jr. Management of 100 consecutive direct carotid-cavernous fistulas: results of treatment with detachable balloons. Neurosurgery. 1995. 36:239–245.5. Luo CB, Teng MM, Chang FC, Chang CY. Transarterial balloon-assisted n-butyl-2-cyanoacrylate embolization of direct carotid cavernous fistulas. AJNR Am J Neuroradiol. 2006. 27:1535–1540.6. Yoshida K, Melake M, Oishi H, Yamamoto M, Arai H. Transvenous embolization of dural carotid cavernous fistulas: a series of 44 consecutive patients. AJNR Am J Neuroradiol. 2010. 31:651–655.
Article7. Archondakis E, Pero G, Valvassori L, Boccardi E, Scialfa G. Angiographic follow-up of traumatic carotid cavernous fistulas treated with endovascular stent graft placement. AJNR Am J Neuroradiol. 2007. 28:342–347.8. Wang C, Xie X, You C, Zhang C, Cheng M, He M, et al. Placement of covered stents for the treatment of direct carotid cavernous fistulas. AJNR Am J Neuroradiol. 2009. 30:1342–1346.
Article9. Lasjaunias P, Santoyo-Vazquez A. Segmental agenesis of the internal carotid artery: angiographic aspects with embryological discussion. Anat Clin. 1984. 6:133–141.
Article10. van Rooij WJ, Sluzewski M, Beute GN. Ruptured cavernous sinus aneurysms causing carotid cavernous fistula: incidence, clinical presentation, treatment, and outcome. AJNR Am J Neuroradiol. 2006. 27:185–189.11. Wang W, Li YD, Li MH, Tan HQ, Gu BX, Wang J, et al. Endovascular treatment of post-traumatic direct carotid-cavernous fistulas: A single-center experience. J Clin Neurosci. 2011. 18:24–28.
Article12. Gemmete JJ, Chaudhary N, Pandey A, Ansari S. Treatment of carotid cavernous fistulas. Curr Treat Options Neurol. 2010. 12:43–53.
Article13. Luo CB, Teng MM, Yen DH, Chang FC, Lirng JF, Chang CY. Endovascular embolization of recurrent traumatic carotid-cavernous fistulas managed previously with detachable balloons. J Trauma. 2004. 56:1214–1220.
Article14. Bavinzski G, Killer M, Gruber A, Richling B. Treatment of post-traumatic carotico-cavernous fistulae using electrolytically detachable coils: technical aspects and preliminary experience. Neuroradiology. 1997. 39:81–85.
Article15. Luo CB, Teng MM, Chang FC, Chang CY. Traumatic indirect carotid cavernous fistulas: angioarchitectures and results of transarterial embolization by liquid adhesives in 11 patients. Surg Neurol. 2009. 71:216–222.
Article16. Li MH, Li YD, Tan HQ, Luo QY, Cheng YS. Treatment of distal internal carotid artery aneurysm with the willis covered stent: a prospective pilot study. Radiology. 2009. 253:470–477.
Article17. Li J, Lan ZG, Xie XD, You C, He M. Traumatic carotid-cavernous fistulas treated with covered stents: experience of 12 cases. World Neurosurg. 2010. 73:514–519.
Article18. Hoit DA, Schirmer CM, Malek AM. Stent graft treatment of cerebrovascular wall defects: intermediate-term clinical and angiographic results. Neurosurgery. 2008. 62:ONS380–ONS388.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Central Retinal Vein Occlusion During Embolization for Carotid Cavernous Sinus Fistula
- Endovascular Graft-Stent Placement for Treatment of Traumatic Carotid Cavernous Fistulas
- Treatment of Traumatic Carotid-Cavernous Fistulas using Debrun's Detachable Balloons
- GDC(Guglielmi Detachable Coil) Embolization Used in Carotid-Cavernous Fistula Incompletely Occluded by Detachable Balloon
- Transarterial Guglielmi Detachable Coils Embolization with Stenting for the Treatment of a Traumatic Carotid Cavernous Fistula: Case Report
