Streptococcus Constellatus Community Acquired Pneumonia with Subsequent Isolated Pulmonic Valve Endocarditis and Abscess Formation in a Structurally Normal Heart
- Affiliations
-
- 1Department of Cardiac Sciences, Libin Cardiovascular Institute, Foothills Medical Center, University of Calgary, Calgary, Alberta, Canada. tarek.elhussein@albertahealthservices.ca
- KMID: 2177468
- DOI: http://doi.org/10.4250/jcu.2014.22.2.91
Abstract
- Pulmonic valve infective endocarditis in isolation is a rare clinical entity. The formation of an abscess in the right ventricular outflow tract as a consequence of vegetations affecting the pulmonic valve in a structurally normal heart is extremely rare and has not been reported. We report a case of isolated pulmonic valve endocarditis complicated by a regional abscess formed within the right ventricular outflow tract caused by Streptococcus Constellatus (S. Constellatus), a member of the Streptococcus Milleri group in a young male whose risk factor was alcohol abuse and he was treated medically, a comprehensive literature review on the subject is also reported. Our case is the first reported in literature with infective endocarditis caused by S. Constellatus affecting the pulmonic valve, and the first with pulmonic valve endocarditis and perivalvular abscess formation in a structurally normal heart.
MeSH Terms
Figure
-

Fig. 1 Transthoracic echocardiogram. Left parasternal short axis view at the level of the aortic valve showing (arrow) large sized vegetation attached to the pulmonic valve.
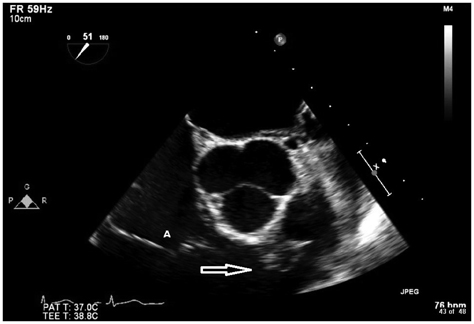
Fig. 2 Transoesophageal echocardiogram. Mid-oesophageal short axis view at the level of the aortic valve showing (arrow) large sized vegetation attached to the right ventricular outflow tract side of the pulmonic valve. A: tricuspid valve appears normal in structure.
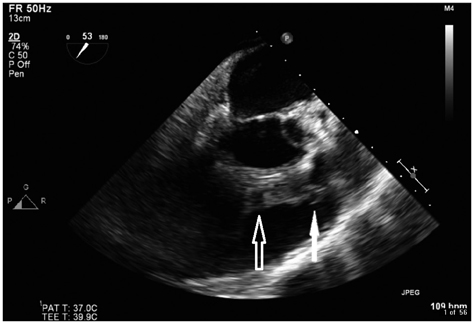
Fig. 3 Transoesophageal echocardiogram. Mid-oesophageal right ventricular outflow view showing large sized vegetations attached to the right ventricular outflow tract (RVOT) side of the pulmonic valve (solid arrow). An abscess within the posterior wall of the RVOT, note the echo free spaces within (open arrow).
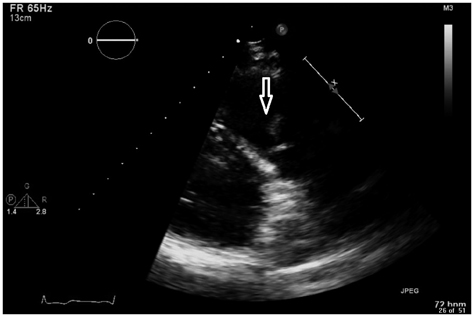
Fig. 4 Transthoracic echocardiogram. Left parasternal right ventricular outflow tract (RVOT) view showing moderate sized chronic healed vegetation attached to the pulmonic valve. No abscess is identified in the RVOT (arrow).
Reference
-
1. Cassling RS, Rogler WC, McManus BM. Isolated pulmonic valve infective endocarditis: a diagnostically elusive entity. Am Heart J. 1985; 109(3 Pt 1):558–567.
Article2. Ramadan FB, Beanlands DS, Burwash IG. Isolated pulmonic valve endocarditis in healthy hearts: a case report and review of the literature. Can J Cardiol. 2000; 16:1282–1288.3. Schroeder RA. Pulmonic valve endocarditis in a normal heart. J Am Soc Echocardiogr. 2005; 18:197–198.
Article4. Cremieux AC, Witchitz S, Malergue MC, Wolff M, Vittecocq D, Vilde JL, Frottier J, Valere PE, Gibert C, Saimot AG. Clinical and echocardiographic observations in pulmonary valve endocarditis. Am J Cardiol. 1985; 56:610–613.
Article5. Habib G, Badano L, Tribouilloy C, Vilacosta I, Zamorano JL, Galderisi M, Voigt JU, Sicari R, Cosyns B, Fox K, Aakhus S. European Association of Echocardiography. Recommendations for the practice of echocardiography in infective endocarditis. Eur J Echocardiogr. 2010; 11:202–219.
Article6. Moreira D, Correia E, Rodrigues B, Santos L, Capelo J, Abreu L, Nunes L, Oliveira-Santos J. Isolated pulmonary valve endocarditis in a normal heart. Rev Port Cardiol. 2012; 31:615–617.
Article7. Hamza N, Ortiz J, Bonomo RA. Isolated pulmonic valve infective endocarditis: a persistent challenge. Infection. 2004; 32:170–175.
Article8. Graf S, Binder T, Heger M, Apfalter P, Simon N, Winkler S. Isolated endocarditis of the pulmonary valve caused by Pasteurella multocida. Infection. 2007; 35:43–45.
Article9. Willcox MD. Potential pathogenic properties of members of the "Streptococcus milleri" group in relation to the production of endocarditis and abscesses. J Med Microbiol. 1995; 43:405–410.
Article10. Ejima K, Ishizuka N, Tanaka H, Tanimoto K, Shoda M, Kasanuki H. [Prosthetic valve endocarditis caused by Streptococcus constellatus infection complicated with perivalvular abscess: serial observation by transesophageal echocardiography: a case report]. J Cardiol. 2003; 42:129–133.11. Pedersen WR, Walker M, Olson JD, Gobel F, Lange HW, Daniel JA, Rogers J, Longe T, Kane M, Mooney MR, et al. Value of transesophageal echocardiography as an adjunct to transthoracic echocardiography in evaluation of native and prosthetic valve endocarditis. Chest. 1991; 100:351–356.
Article12. Jacob S, Tong AT. Role of echocardiography in the diagnosis and management of infective endocarditis. Curr Opin Cardiol. 2002; 17:478–485.
Article13. Daniel WG, Mügge A, Martin RP, Lindert O, Hausmann D, Nonnast-Daniel B, Laas J, Lichtlen PR. Improvement in the diagnosis of abscesses associated with endocarditis by transesophageal echocardiography. N Engl J Med. 1991; 324:795–800.
Article14. Deng H, Ma Y, Zhai H, Miao Q. Surgical valve repair of isolated pulmonary valve endocarditis. Interact Cardiovasc Thorac Surg. 2013; 16:384–386.
Article15. Dayan V, Gutierrez F, Cura L, Soca G, Lorenzo A. Two cases of pulmonary homograft replacement for isolated pulmonary valve endocarditis. Ann Thorac Surg. 2009; 87:1954–1956.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical and Echocardiographic Features of Pulmonic Valve Endocarditis in patients with Ventricular Septal Defect
- Infective endocarditis involving an apparently structurally normal valve: new epidemiological trend?
- A Case of Staphylococcal Tricuspid Valve Endocarditis With Para-Aortic Abscess in a Patient With Bicuspid Aortic Valve
- A case of gas gangrene caused by Streptococcus constellatus
- Endocarditis Caused by Community-Acquired Klebsiella pneumoniae Infection - A Case Report -
