Massive Cardiomegaly due to Dilated Cardiomyopathy Causing Bronchial Obstruction in an Infant
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, The Catholic University of Korea, Seoul, Korea. jeany@catholic.ac.kr
- KMID: 2177464
- DOI: http://doi.org/10.4250/jcu.2014.22.2.84
Abstract
- Dilated cardiomyopathy (DCMP) remains a life threatening disease in young patients and is often difficult to differentiate from myocarditis. Early recognition and treatment of DCMP are crucial for good prognoses in this patient population. The clinical course of patients with DCMP that result in cardiogenic shock varies according to the etiology as well as patient age. The volumetric expansion of the enlarged heart can compress adjacent structures causing a number of related symptoms, especially in infants with soft cartilaginous bronchi. Therapeutic strategies for treating these issues vary according to the type of complication encountered. We report a case of severe DCMP with sudden onset of massive cardiomegaly with heart failure complicated by bronchial obstruction in an infant.
MeSH Terms
Figure
-

Fig. 1 Chest roentgenography obtained shortly after premature birth (A), on admission after the onset of shock with cardiomegaly and unilateral white out of entire left lung field (B), and three months after the onset of symptoms checked at out patient clinic in which cardiomegaly renders cardiac sillhouette vague (C), and gradual improvement of cardiomegaly after 6 (D) and 12 months (E).
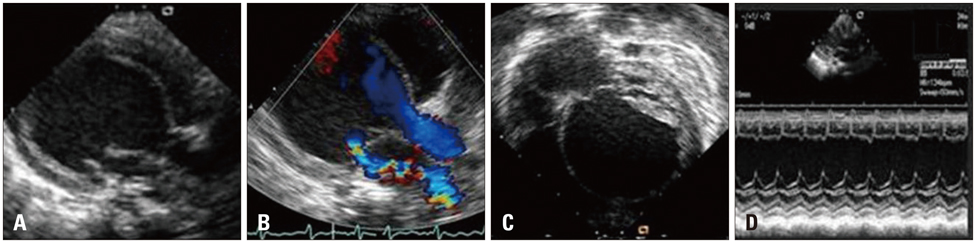
Fig. 2 Initial echocardiography showing a markedly dilated left ventricle (LV) on the parasternal long axis view (A) with mitral valve regurgitation through a coaptation site without significant left atrial enlargement (B). Spherical LV on the subcostal 4-chamber view (C) with increased EPSS on M-mode echocardiography (D).

Fig. 3 Chest CT showing the spherically enlarged left ventricle occupying the entire left intrathoracic space (A and B) with left main stem bronchus compression between the left atrium and descending aorta (C). Three dimensional reconstruction of the airway showing external compression of the left main stem bronchus (D).
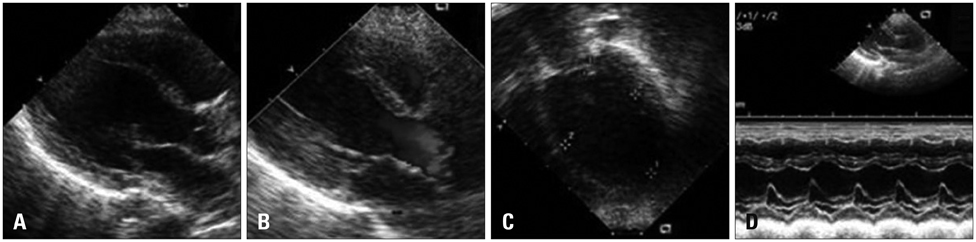
Fig. 4 Echocardiographic images correspondingly matched with Fig. 2 each showing normal ellipsoid left ventricle configuration after 12 months of treatment on the parasternal long axis view without mitral valve regurgitation or left atrial enlargement (A and B) and on the apical 4-chamber view (C) with improved wall motion on M-mode echocardiography (D).
Reference
-
1. Harmon WG, Sleeper LA, Cuniberti L, Messere J, Colan SD, Orav EJ, Towbin JA, Wilkinson JD, Lipshultz SE. Treating children with idiopathic dilated cardiomyopathy (from the Pediatric Cardiomyopathy Registry). Am J Cardiol. 2009; 104:281–286.
Article2. Oh JH, Hong YM, Choi JY, Kim SJ, Jung JW, Sohn S, Hyun MC, Noh CI, Lee JW, Park IS. Idiopathic cardiomyopathies in Korean children. - 9-Year Korean Multicenter Study-. Circ J. 2011; 75:2228–2234.
Article3. Shaddy RE, Boucek MM, Hsu DT, Boucek RJ, Canter CE, Mahony L, Ross RD, Pahl E, Blume ED, Dodd DA, Rosenthal DN, Burr J, LaSalle B, Holubkov R, Lukas MA, Tani LY. Pediatric Carvedilol Study Group. Carvedilol for children and adolescents with heart failure: a randomized controlled trial. JAMA. 2007; 298:1171–1179.
Article4. Gazit AZ, Oren PP. Pharmaceutical management of decompensated heart failure syndrome in children: current state of the art and a new approach. Curr Treat Options Cardiovasc Med. 2009; 11:403–409.
Article5. Leung RS, Bradley TD. Long term treatment of refractory congestive heart failure by continuous positive airway pressure. Can J Cardiol. 1999; 15:1009–1012.6. Kussman BD, Geva T, McGowan FX. Cardiovascular causes of airway compression. Paediatr Anaesth. 2004; 14:60–74.
Article7. Park SH, Park SY, Kim NK, Park SJ, Park HK, Park YH, Choi JY. Bronchial compression in an infant with isolated secundum atrial septal defect associated with severe pulmonary arterial hypertension. Korean J Pediatr. 2012; 55:297–300.
Article8. Dailey ME, O'Laughlin MP, Smith RJ. Airway compression secondary to left atrial enlargement and increased pulmonary artery pressure. Int J Pediatr Otorhinolaryngol. 1990; 19:33–44.
Article9. Sagy M, Silver P, Nimkoff L, Zahtz G, Amato JJ, Bierman FZ. Pediatric intrathoracic large airway obstruction: diagnostic and therapeutic considerations. Pediatr Emerg Care. 1994; 10:351–358.10. Goo HW. Cardiac MDCT in children: CT technology overview and interpretation. Radiol Clin North Am. 2011; 49:997–1010.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Dilated Cardiomyopathy in a 2 Month-Old Infant: A Severe Form of Hypocalcemia With Vitamin D Deficient Rickets
- A Case of Dilated Cardiomyopathy with Massive Left Ventricular Thrombus after Use of a Sibutramine-Containing Slimming Product
- Echocardiographic Study of the Aortic Root and Valve in Dilated Cardiomyopathy
- Duchenne Muscular Dystrophy Complicated With Dilated Cardiomyopathy and Cerebral Infarction
- A Case of Normalized Hypertrophic Cardiomyopathy after Removal of Pheochromocytoma
