J Cardiovasc Ultrasound.
2012 Jun;20(2):108-111. 10.4250/jcu.2012.20.2.108.
Multiple Fistula Emptying into the Left Ventricle through the Entire Left Ventricular Wall
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Kyungpook National University Hospital, Daegu, Korea. ddhyang@knu.ac.kr
- KMID: 2177376
- DOI: http://doi.org/10.4250/jcu.2012.20.2.108
Abstract
- Coronary artery fistulae are usually identified during invasive coronary angiographies. However, in this case, we made the early detection of coronary artery fistulae during non-invasive transthoracic echocardiography, by demonstrating diastolic multiple abnormal color Doppler flows on the entire left ventricular walls including left ventricular free wall, interventricular septum and apex, which were mimicking firecracker on the whole left ventricle. Fistulous communication from the coronary artery to the left ventricle is rare. Moreover, a case of multiple coronary fistulae emptying into the left ventricle through the entire left ventricular walls including left ventricular free wall, interventricular septum and apex is uncommon. We report a case of a 31-year-old woman who was diagnosed with multiple fistula communicating with entire left ventricular wall.
Keyword
MeSH Terms
Figure
-

Fig. 1 Electrocardiography showing biphasic T wave in lead V1-3.

Fig. 2 Transthoracic parasternal long axis, short axis and apical four chamber view: Note the sinusoidal mesh like structure in the basal anteroseptum wall, and multiple sparkling color Doppler flows through the entire left ventricular walls during diastole.
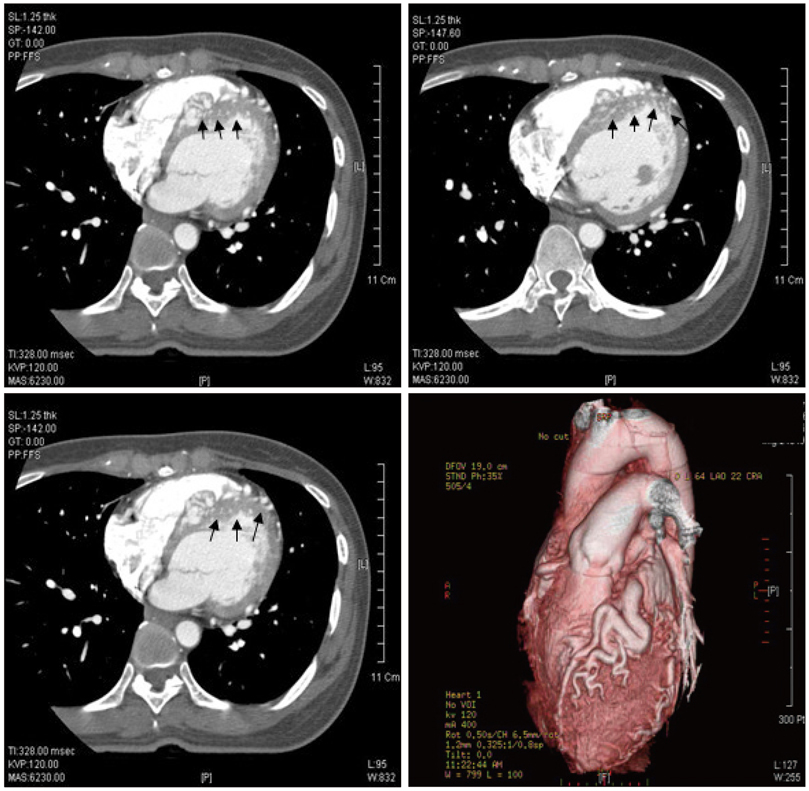
Fig. 3 The computerized tomographic angiography showing multiple fistula draining into left ventricular cavity through interventricular septum and apex (arrows): Coronary artery had markedly tortuous and dilated morphology from left main coronary artery to left anterior descending artery.
Reference
-
1. Parra-Bravo JR, Beirana-Palencia LG. [Right coronary artery fistula opening into right ventricle. Echocardiographic findings and interventional management. Report of a case]. Arch Cardiol Mex. 2003. 73:205–211.2. Chen ML, Lo HS, Su HY, Chao IM. Coronary artery fistula: assessment with multidetector computed tomography and stress myocardial single photon emission computed tomography. Clin Nucl Med. 2009. 34:96–98.3. Abelin AP, Sarmento-Leite R, Quadros AS, Gottschall CAM. Coronary fistula. Rev Bras Cardiol Invas. 2008. 16:242–243.4. Hobbs RE, Millit HD, Raghavan PV, Moodie DS, Sheldon WC. Coronary artery fistulae: a 10-year review. Cleve Clin Q. 1982. 49:191–197.
Article5. Levin DC, Fellows KE, Abrams HL. Hemodynamically significant primary anomalies of the coronary arteries. Angiographic aspects. Circulation. 1978. 58:25–34.
Article6. Sherwood MC, Rockenmacher S, Colan SD, Geva T. Prognostic significance of clinically silent coronary artery fistulas. Am J Cardiol. 1999. 83:407–411.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Coronary Artery Fistula Draining into the Left Ventricle
- Abnormal Motion of Left Ventricular Posterior Wall and Aortic Root Posterior Wall in Patients with Left Ventricular Hypertrophy: An Echocardiographic Study
- Aneurysm of the inferobasal wall and ventricular septal rupture complicated with inferior myocardial infarction
- The Changes of the Velocities of the Motions of the Posterior Aortic Wall in Hypertensive Heart Disease
- Abnormality of Regional Wall Motion of the Left Ventricle in Children with Ventricular Diastolic Overload
