Chest Wall Lipogranuloma after Hydrogel Implant Rupture: Case Report
- Affiliations
-
- 1Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. bkhan@skku.edu
- 2Department of Pathology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 3Department of Plastic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2175615
- DOI: http://doi.org/10.13104/imri.2015.19.3.191
Abstract
- We present a 53-year-old woman with a large chest wall mass in the interpectoral space, which was eventually confirmed as a lipogranuloma resulting from hydrogel implant rupture. Ultrasonography (US) showed reduced implant volume with surrounding peri-implant fluid collection, suggesting the possibility of implant rupture. A heterogeneously hypoechoic mass was found between the pectoralis major and minor muscles adjacent to the ruptured implant. On magnetic resonance imaging (MRI), there was a large mass in the left interpectoral space of the upper inner chest wall. The mass showed slightly high signal intensity (SI) on pre-contrast T1-weighted image (WI) with mixed iso and high SI on T2-WI. The signal of the mass was suppressed using the water suppression technique but not with the fat suppression technique on T2-WI. The mass showed diffuse enhancement upon contrast enhancement. The enhancing kinetics showed persistent enhancement pattern. US-guided core needle biopsy revealed a lipogranuloma and removal confirmed a ruptured PIP hydrogel implant.
Keyword
MeSH Terms
Figure
-
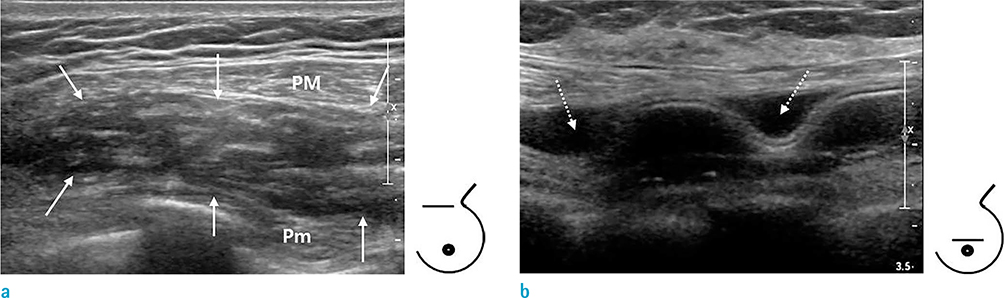
Fig. 1 Transverse ultrasonography of left upper chest wall (a) and breast area (b). (a) Ultrasonography shows a 5-cm-sized, ill-defined heterogeneously echogenic mass (arrows) between pectoralis major (PM) and minor (Pm) muscle, superior to the implant. (b) The implant shows a reduced volume with peri-implant fluid collection (dotted arrows).

Fig. 2 Axial MRI of the breast. On MRI at the mass level, an 8 × 8 × 2 cm mass in the left interpectoral space of upper inner chest wall (arrows) shows slightly high signal intensity (SI) compared to the muscle in pre-contrast T1-weighted image (WI) and it shows a mixture of iso and high SI on T2-WI. The signal of the mass is suppressed by water suppressed T2-WI but not by fat suppressed T2-WI. The mass shows diffuse enhancement by contrast enhanced (CE) T1-WI.
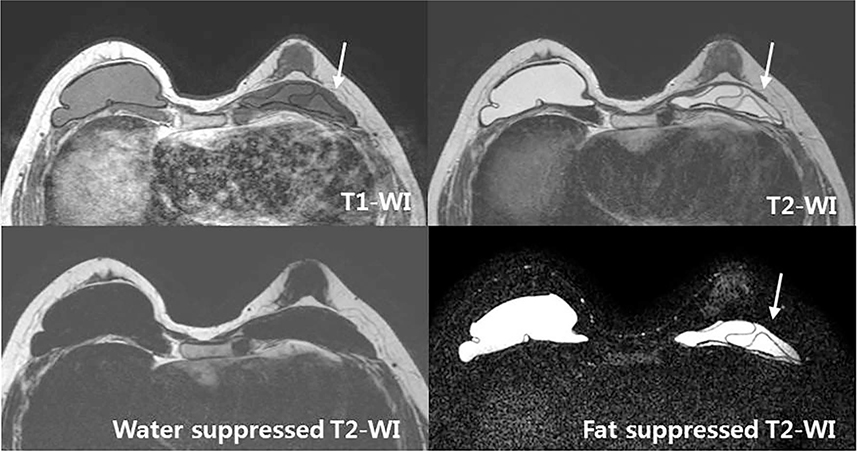
Fig. 3 On MRI at the implant level, the left subpectoral implant is collapsed with a linguine sign, representing a rupture (arrows). The SI of the implant is low on T1-WI and high in T2-WI and is suppressed by water suppressed T2-WI but not by fat suppressed T2-WI, which is compatible with hydrogel implants and not with silicone implants.

Fig. 4 (Upper) The core biopsy specimen consists almost entirely of homogenous lipid-containing macrophages without extracellular fat vacuoles (Hematoxylin & Eosin, × 400). (Lower) Intracellular fat components show positive Sudan black B staining (arrows) (Sudan black B, × 400).
Reference
-
1. Lee CJ, Park JH, Park IS, Lee SI. A case report of prefilled polysaccharide hydrogel breast implant rupture: clinical, MRI, and pathologic findings. Aesthetic Plast Surg. 2004; 28:401–404.2. Choi JJ, Lee JH, Kang BJ, et al. Clinical and imaging characteristics of Polyimplant Prosthesis hydrogel breast implants. J Comput Assist Tomogr. 2010; 34:449–455.3. Adams TS, Crook T, Cadier MA. A late complication following the insertion of hydrogel breast implants. J Plast Reconstr Aesthet Surg. 2007; 60:210–212.4. O'Neill JK, Rigby H, Kenealy JM. Leakage and osmotic shifts in PIP Hydrogel implants. A case demonstrating increase and decrease of implant volume in the same patient. J Plast Reconstr Aesthet Surg. 2008; 61:1122–1123.5. Lee HH, Park SH, Choi HY, Park HK. Lipogranuloma with osseous metaplasia in the breast that developed after "Bu-Hwang" oriental medicine treatment. Yonsei Med J. 2011; 52:373–376.6. Yang BT, Liu YJ, Wang YZ, Wang XY, Wang ZC. CT and MR imaging findings of periorbital lipogranuloma developing after endoscopic sinus surgery. AJNR Am J Neuroradiol. 2012; 33:2140–2143.7. Motoori K, Takano H, Ueda T, Ishihara M. Sclerosing lipogranuloma of male genitalia: CT and MR images. J Comput Assist Tomogr. 2002; 26:138–140.8. Hyakusoku H, Ogawa R, Ono S, Ishii N, Hirakawa K. Complications after autologous fat injection to the breast. Plast Reconstr Surg. 2009; 123:360–370.9. Veber M, Tourasse C, Toussoun G, Moutran M, Mojallal A, Delay E. Radiographic findings after breast augmentation by autologous fat transfer. Plast Reconstr Surg. 2011; 127:1289–1299.10. Kim H, Yang EJ, Bang SI. Bilateral liponecrotic pseudocysts after breast augmentation by fat injection: a case report. Aesthetic Plast Surg. 2012; 36:359–362.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Rupture of Breast Implants after Augmentation Mammoplasty: A Case Report of Simultaneous Intra-extracapsular Rupture
- Clinical Features after Rupture of Hydrogel Breast Implants - MDbP206
- Complication of Augmentation Mammoplasty using Polysaccharide Hydrogel Breast implant: Two Cases Report
- Infected Sclerosing Lipogranuloma after Hernioplasty: Ultrasonographic and MRI Findings
- Subconjunctival Lipogranuloma with Orbital Dermoid Cyst
