Cerebellar Embolization in Patients with Heart Murmur
- Affiliations
-
- 1The Heart Research Center Nominated by Korea Ministry of Health and Welfare, Gwangju, Korea. mhjeong@chonnam.ac.kr
- KMID: 2172245
- DOI: http://doi.org/10.4068/cmj.2011.47.1.45
Abstract
- A 76-year-old female present to the emergency department with dysarthria, dizziness, dyspnea. The patient had hypertension and atrial fibrillation. Brain MRI revealed right cerebellar infarction. Transthoracic echocardiography showed a large round mass in the left atrium. Transesophageal echocardiography showed large complex echogenic round mass lesion attached on left atrial side of interatrial septum. Coronary angiogram revealed round movable mass lesion in left atrium with feeding arteries originated from right coronary artery. She underwent removal of mass and Maze operation, and pathologic finding was compatible with myxoma.
Keyword
MeSH Terms
Figure
-
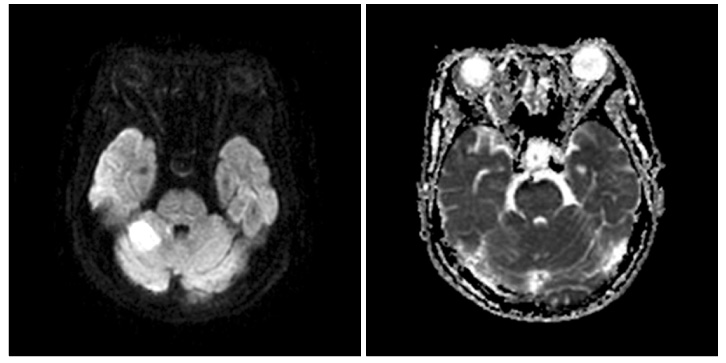
FIG. 1 Axial T1-weighted image showed a high signal intensity lesion (Left) and the T2-weighted image showed a low signal intensity lesion (Right) in the right cerebellum.
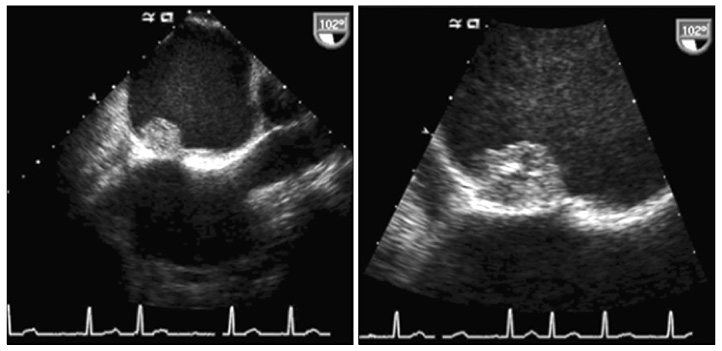
FIG. 2 Transesophageal echocardiography showed a complex, echogenic, round mass lesion in the left atrial side of the interatrial septum.

FIG. 3 Left and Right: coronary angiogram revealed no significant stenosis but a round mass lesion in the left atrium with feeding arteries originating from the conus branch and the atrioventricular nodal artery of the right coronary artery.

FIG. 4 Hematoxylin-eosin staining showed an acid mucopoly-saccharide-rich stroma composed of a myxoid matrix and polygonal cells with scant eosinophilic cytoplasm scattered throughout the matrix. Low power field (×40).
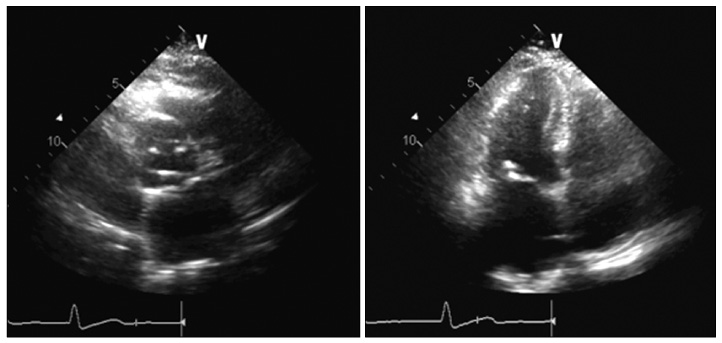
FIG. 5 Follow-up transthoracic echocardiography after surgery showed no remnant mass lesion in the left atrium.
Reference
-
1. Reynen K. Cardiac myxomas. N Engl J Med. 1995. 333:1610–1617.
Article2. Mundi A. Images in clinical medicine. Large atrial myxoma. N Engl J Med. 2009. 361:e51.3. Alam M, Sun I. Transesophageal echocardiographic evaluation of left atrial mass lesions. J Am Soc Echocardiogr. 1991. 4:323–330.
Article4. Burke A, Jeudy J Jr, Virmani R. Cardiac tumours: an update: cardiac tumours. Heart. 2008. 94:117–123.5. Alam M. Pitfalls in the echocardiographic diagnosis of intracardiac and extracardiac masses. Echocardiography. 1993. 10:181–191.
Article6. Kuroczyński W, Peivandi AA, Ewald P, Pruefer D, Heinemann M, Vahl CF. Cardiac myxomas: short- and long-term follow-up. Cardiol J. 2009. 16:447–454.7. Bhan A, Mehrotra R, Choudhary SK, Sharma R, Prabhakar D, Airan B, et al. Surgical experience with intracardiac myxomas: long-term follow-up. Ann Thorac Surg. 1998. 66:810–813.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Echocardiographic Findings in Children with Heart Murmur Detected at Mass Health Screening in Kyeong-Nam Province
- Persistent Trigeminal Artery with a Cerebellar Branch and Trigeminal-Cavernous Fistula from Ruptured Aneurysm: Transarterial Coil Embolization
- Evaluation and diagnostic approach for heart murmurs in children
- Coil Embolization of Ruptured Thrombosed Distal Superior Cerebellar Artery Aneurysm: A Case Report
- An Adult Case of Internal Mammary Arterio-Venous Fistula
