Acute Myocardial Infarction Occurred in Multivessel Disease Including Chronic Total Occlusion
- Affiliations
-
- 1Department of Internal Medicine, Yeungnam University Medical Center, Daegu, Korea.
- 2Department of Internal Medicine, Kyungpook National University Hospital, Daegu, Korea.
- 3Department of Internal Medicine, National Cancer Center, Seoul, Korea.
- 4Department of Cardiology, Pohang Stroke and Spine Hospital, Pohang, Korea. hosanna7835@hanmail.net
- KMID: 2171352
- DOI: http://doi.org/10.12771/emj.2015.38.3.133
Abstract
- Simultaneous multi-vessel acute myocardial infarction is rare and has poor prognosis. We report a 70-year-old Korean man with an anteroseptal wall ST-elevation myocardial infarction presenting as ventricular tachycardia, sudden cardiac arrest and cardiogenic shock. After successful cardiopulmonary resuscitation, a coronary angiogram revealed three-vessel coronary disease; simultaneous total occlusions of the proximal left anterior descending artery (LAD) and the proximal left circumflex artery (LCX), and chronic total occlusion of the proximal right coronary artery. Primary percutaneous coronary intervention (PCI) of the LAD and LCX was successful and an intra-aortic balloon pump was inserted. Despite the timely and successful PCI result, he died on the 58th day in the hospital due to pneumonia with multiple organ failure.
MeSH Terms
Figure
-
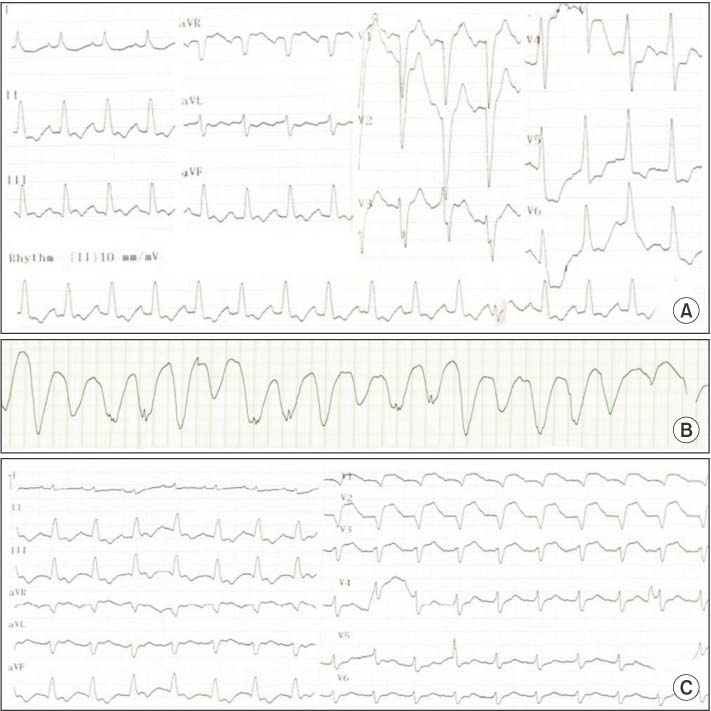
Fig. 1 Electrocardiogram (ECG). (A) Initial ECG in the emergency room shows ST elevation in aVR and non-specific ST-T change. (B) Six hours later, a sudden pulseless VT is detected. (C) After successful resuscitation, ECG shows ST-segment elevation in the anteroseptal wall.
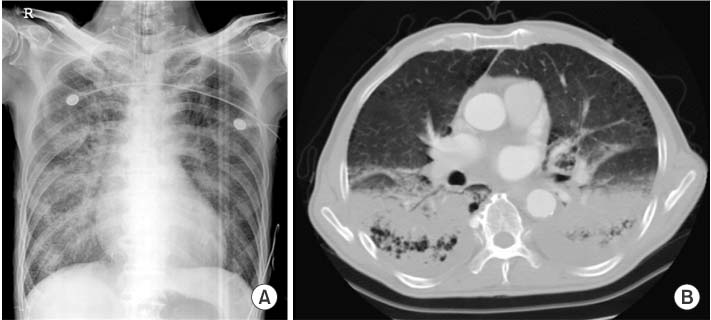
Fig. 2 Chest radiography (A) and chest computed tomography scan (B). These show that both lower lobes had pneumonia.
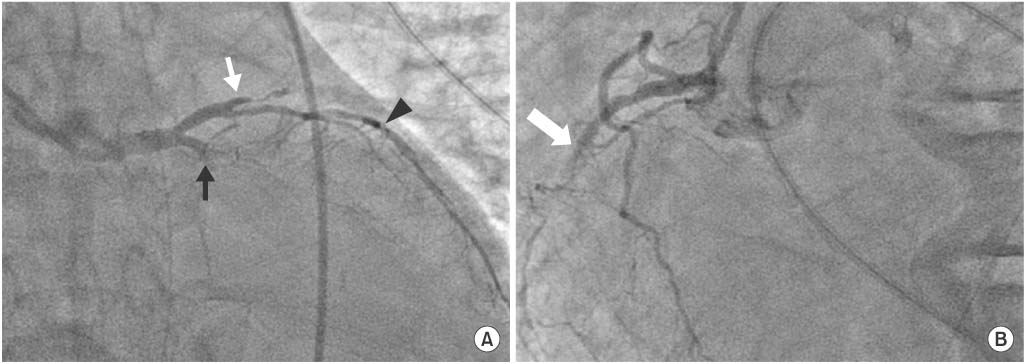
Fig. 3 Initial coronary angiogram. (A) Caudal view of left system angiogram shows total occlusion of the proximal left anterior descending artery (white arrow) and left circumflex artery (black arrow). There is seen diagonal artery (arrow head) with thrombosis in myocardial infarction flow II. (B) Left anterior oblique view of coronary angiogram shows total occlusion of the proximal RCA (arrow).
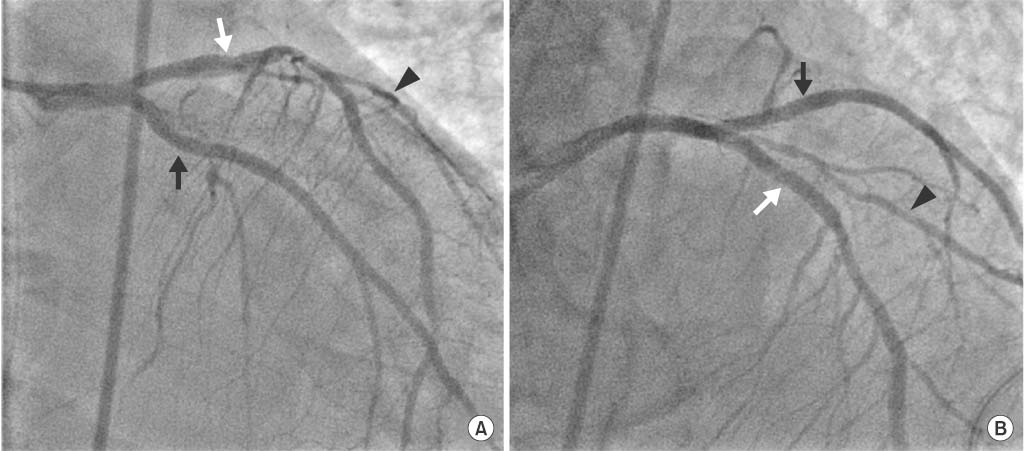
Fig. 4 Coronary angiogram after the intervention. (A) Caudal view of left system angiogram. (B) Left anterior oblique cranial view of coronary angiogram. Successful implantations of everolimus-eluting stent at the proximal left anterior descending artery (white arrow) and the proximal left circumflex artery (black arrow) results in thrombosis in myocardial infarction (TIMI) flow III. Also seen is diagonal artery (arrow head) with TIMI flow II.
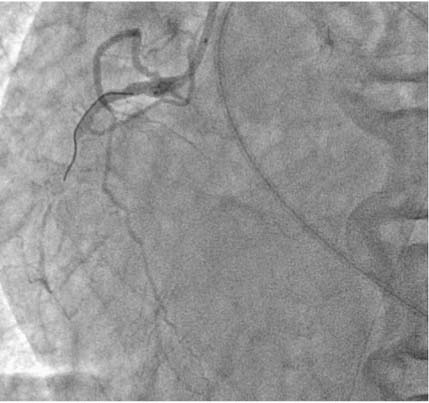
Fig. 5 Left anterior oblique view of coronary angiogram. Stent implantation is failed as the guidewire could not pass through the right coronary artery lesion.
Reference
-
1. Vincent GM, Anderson JL, Marshall HW. Coronary spasm producing coronary thrombosis and myocardial infarction. N Engl J Med. 1983; 309:220–223.2. Sia SK, Huang CN, Ueng KC, Wu YL, Chan KC. Double vessel acute myocardial infarction showing simultaneous total occlusion of left anterior descending artery and right coronary artery. Circ J. 2008; 72:1034–1036.3. De Felice F, Fiorilli F, Parma A, Musto C, Nazzaro MS, Confessore P, et al. Effect of multivessel coronary artery disease with or without a concomitant chronic total occlusion on 1-year survival in patients treated with rescue angioplasty. J Invasive Cardiol. 2013; 25:64–68.4. Valenti R, Migliorini A, Signorini U, Vergara R, Parodi G, Carrabba N, et al. Impact of complete revascularization with percutaneous coronary intervention on survival in patients with at least one chronic total occlusion. Eur Heart J. 2008; 29:2336–2342.5. Kosuge M, Uchida K, Imoto K, Isoda S, Karube N, Ebina T, et al. Prognostic Value of ST-Segment Elevation in Lead aVR in Patients With Type A Acute Aortic Dissection. J Am Coll Cardiol. 2015; 65:2570–2571.6. Mahmoud A, Saad M, Elgendy IY. Simultaneous multi-vessel coronary thrombosis in patients with ST-elevation myocardial infarction: a systematic review. Cardiovasc Revasc Med. 2015; 16:163–166.7. Tan IL, Tan HC, Teo SG, Lim YT. Simultaneous thromboses of multiple coronary arteries in acute myocardial infarction. Singapore Med J. 2006; 47:240–242.8. Glueck CJ, Fontaine RN, Gupta A, Alasmi M. Myocardial infarction in a 35-year-old man with homocysteinemia, high plasminogen activator inhibitor activity, and resistance to activated protein C. Metabolism. 1997; 46:1470–1472.9. Williams MJ, Restieaux NJ, Low CJ. Myocardial infarction in young people with normal coronary arteries. Heart. 1998; 79:191–194.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Concurrent Chronic Total Occlusion in a Non-Infarct Artery Strongly Associate With Poor Long-Term Prognosis in Patients With Acute Myocardial Infarction and Multivessel Coronary Disease
- Two Cases of Multivessel Coronary Artery Ectasias Resulting in Acute Inferior Myocardial Infarction
- Two Cases of Complications during Percutaneous Coronary Intervention for Myocardial Infarction in Patients with Concurrent Chronic Total Occlusion in an Emergency Setting
- Acute Myocardial Infarction with Simultaneous Thrombosis of Multiple Coronary Arteries
- Impact of Multivessel Coronary Disease With Chronic Total Occlusion on One-Year Mortality in Patients With Acute Myocardial Infarction
