Giant plunging ranula: a case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Radiology and Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea. future3@snu.ac.kr
- 2Department of Oral and Maxillofacial Radiology, School of Dentistry, Kyungpook National University, Daegu, Korea.
- 3Department of Periodontology, School of Dentistry, Kyungpook National University, Daegu, Korea.
- 4Department of Oral and Maxillofacial Radiology, BK21 Craniomaxillofacial Life Science, and Dental Research Institute, School of Dentistry, Seoul National University, Seoul, Korea.
- KMID: 2167448
- DOI: http://doi.org/10.5624/isd.2013.43.1.55
Abstract
- A ranula is a bluish, transparent, and thin-walled swelling in the floor of the mouth. They originate from the extravasation and subsequent accumulation of saliva from the sublingual gland. Ranulas are usually limited to the sublingual space but they sometimes extend to the submandibular space and parapharyngeal space, which is defined as a plunging ranula. A 21-year-old woman presented with a complaint of a large swelling in the left submandibular region. On contrast-enhanced CT images, it dissected across the midline, and extended to the parapharyngeal space posteriorly and to the submandibular space inferiorly. Several septa and a fluid-fluid level within the lesion were also demonstrated. We diagnosed this lesion as a ranula rather than cystic hygroma due to the location of its center and its sublingual tail sign. As plunging ranula and cystic hygroma are managed with different surgical approaches, it is important to differentiate them radiologically.
MeSH Terms
Figure
-
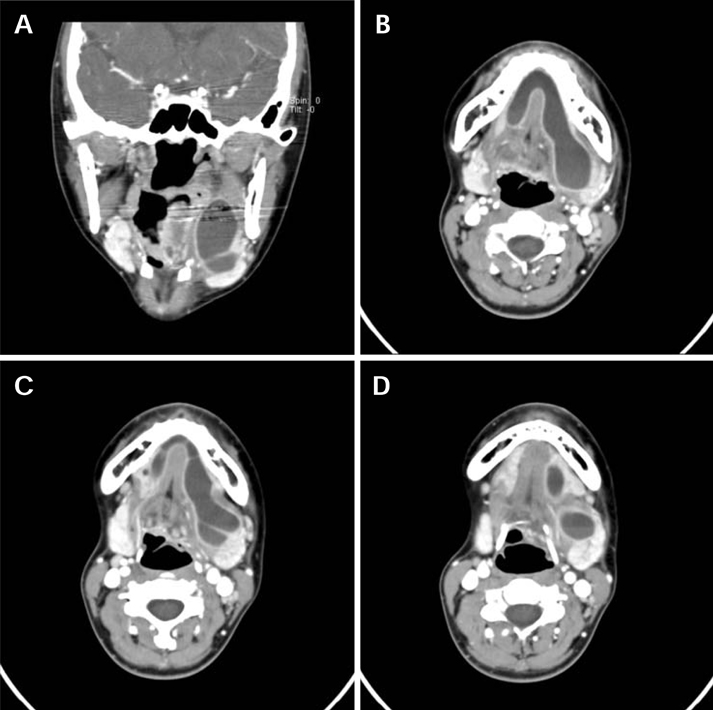
Fig. 1 Contrast-enhanced CT images show a large insinuating, rimenhanced fluid collection occupying both sublingual spaces. A. A coronal contrast-enhanced CT image shows the superior extension of the lesion into the parapharyngeal space and inferior displacement of the left submandibular gland by the lesion. B. An axial contrast-enhanced CT image demonstrates a horseshoe shaped fluid attenuation lesion. C. A contiguous axial contrast-enhanced CT image at a level slightly inferior to (B). Note several subtle septa within the lesion. D. A contiguous axial contrast-enhanced CT image at a level slightly inferior to (C) reveals a fluid-fluid level.
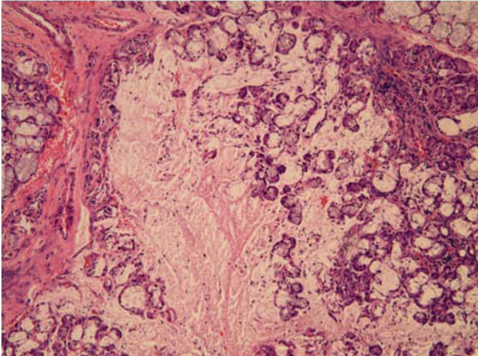
Fig. 2 Ruptured acinar cells are evident in the sublingual gland, which indicates that this cystic lesion is arising from the sublingual gland (H&E stain, ×100).
Reference
-
1. Catone GA, Merrill RG, Henny FA. Sublingual gland mucusescape phenomenon-treatment by excision of sublingual gland. J Oral Surg. 1969. 27:774–786.2. Brunner H. Pathology of ranula. Oral Surg Oral Med Oral Pathol. 1949. 2:1591–1598.
Article3. Harrison JD, Fouad HM, Garrett JR. Variation in the response to ductal obstruction of feline submandibular and sublingual salivary glands and the importance of the innervation. J Oral Pathol Med. 2001. 30:29–34.
Article4. van den Akker HP, Bays RA, Becker AE. Plunging or cervical ranula. Review of the literature and report of 4 cases. J Maxillofac Surg. 1978. 6:286–293.5. Koeller KK, Alamo L, Adair CF, Smirniotopoulos JG. Congenital cystic masses of the neck: radiologic-pathologic correlation. Radiographics. 1999. 19:121–146.6. Rho MH, Kim DW, Kwon JS, Lee SW, Sung YS, Song YK, et al. OK-432 sclerotherapy of plunging ranula in 21 patients: it can be a substitute for surgery. AJNR Am J Neuroradiol. 2006. 27:1090–1095.7. Kurabayashi T, Ida M, Yasumoto M, Ohbayashi N, Yoshino N, Tetsumura A, et al. MRI of ranulas. Neuroradiology. 2000. 42:917–922.
Article8. Bhaskar SN, Bolden TE, Weinmann JP. Pathogenesis of mucoceles. J Dent Res. 1956. 35:863–874.
Article9. Chidzonga MM, Mahomva L. Ranula: experience with 83 cases in Zimbabwe. J Oral Maxillofac Surg. 2007. 65:79–82.
Article10. Afzali P, Mandel L. Right submandibular mass. J Am Dent Assoc. 2009. 140:1381–1383.
Article11. Suresh BV, Vora SK. Huge plunging ranula. J Maxillofac Oral Surg. 2012. 11:487–490.
Article12. Davison MJ, Morton RP, McIvor NP. Plunging ranula: clinical observations. Head Neck. 1998. 20:63–68.
Article13. Coit W, Harnsberger H, Osborn A, Smoker W, Stevens M, Lufkin R. Ranulas and their mimics: CT evaluation. Radiology. 1987. 163:211–216.
Article14. Macdonald AJ, Salzman KL, Harnsberger HR. Giant ranula of the neck: differentiation from cystic hygroma. AJNR Am J Neuroradiol. 2003. 24:757–761.15. Burezq H, Williams B, Chitte SA. Management of cystic hygromas: 30 year experience. J Craniofac Surg. 2006. 17:815–818.16. Zhao YF, Jia Y, Chen XM, Zhang WF. Clinical review of 580 ranulas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004. 98:281–287.
Article17. Harrison JD. Modern management and pathophysiology of ranula: literature review. Head Neck. 2010. 32:1310–1320.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Bilateral Plunging Ranula
- Transoral Drainage of Plunging Ranula using Intraoperative Ultrasonography after Sublingual Gland Resection: A Case Report
- PLUNGING RANULA IN A 4-YEAR-OLD CHILD: REPORT OF A CASE
- Case report of the management of the ranula
- A case report of Plunging ranula with metastatic adenocarcinoma
