Giant malignant insulinoma
- Affiliations
-
- 1Department of Surgery, University Hospital of Patras, Rion, Greece. dimitriskaravias@gmail.com
- 2Division of Endocrinology and Diabetes, Department of Internal Medicine, University Hospital of Patras, Rion, Greece.
- 3Department of Radiology, University Hospital of Patras, Rion, Greece.
- 4Department of Pathology, University Hospital of Patras, Rion, Greece.
- KMID: 2166998
- DOI: http://doi.org/10.4174/astr.2015.88.5.289
Abstract
- Insulinomas are the most common pancreatic neuroendocrine tumors. Most insulinomas are benign, small, intrapancreatic solid tumors and only large tumors have a tendency for malignancy. Most patients present with symptoms of hypoglycemia that are relieved with the administration of glucose. We herein present the case of a 75-year-old woman who presented with an acute hypoglycemic episode. Subsequent laboratory and radiological studies established the diagnosis of a 17-cm malignant insulinoma, with local invasion to the left kidney, lymph node metastasis, and hepatic metastases. Patient symptoms, diagnostic and imaging work-up and surgical management of both the primary and the metastatic disease are reviewed.
Keyword
MeSH Terms
Figure
-
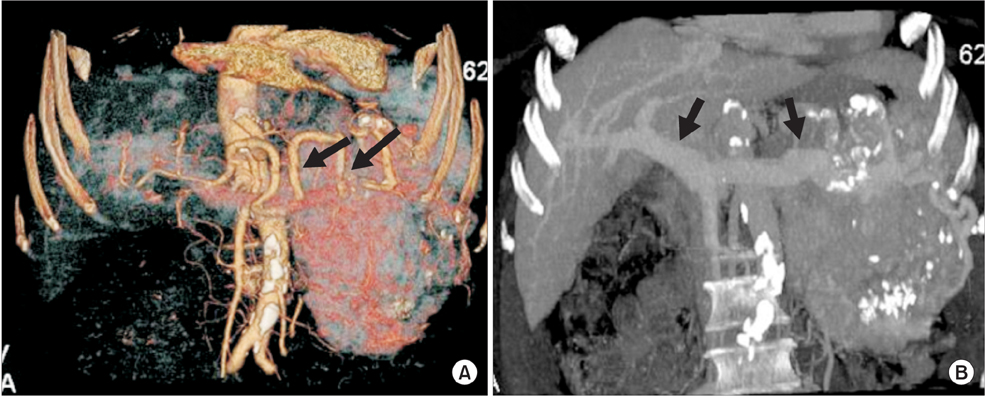
Fig. 1 (A) Coronal volume rendering reformatted image demonstrates patent splenic artery surrounded by tumor (arrows). (B) Coronal maximum intensity projection reformatted image depicting patent portal and splenic vein (arrows).
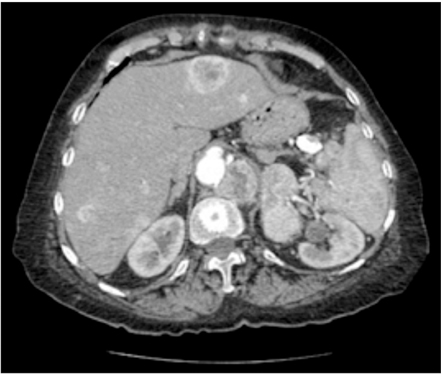
Fig. 2 Post contrast axial CT image during arterial phase. Multiple hypervascular metastases are seen in liver.
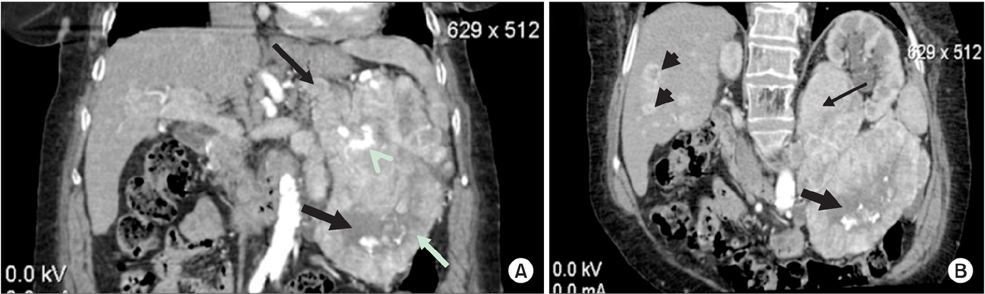
Fig. 3 Post contrast reformatted CT images (A: coronal MPR, B: oblique MPR) during arterial phase. There is heterogeneously enhancing lobulated mass (arrows in A) in pancreatic tail with central necrosis (black block arrow in A). Coarse calcifications are also present within necrotic areas (white arrowhead in A). Large enhancing masses are also evident at level of left renal hilum (arrows in B) and at left retrocrural space (white arrow in A). Multiple hypervascular metastases are seen in liver (block arrowheads in B). MPR, multiplanar reformatting.
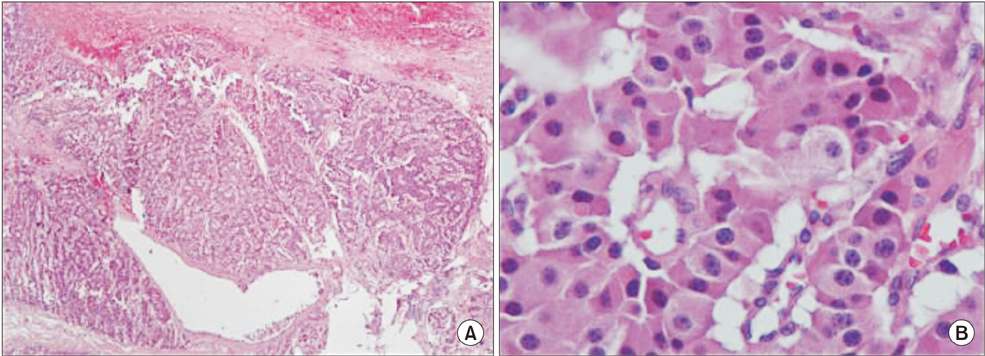
Fig. 4 (A, B) Microphotograph showing section from tumor with acinar pattern (H&E: A, ×100; B, ×400).
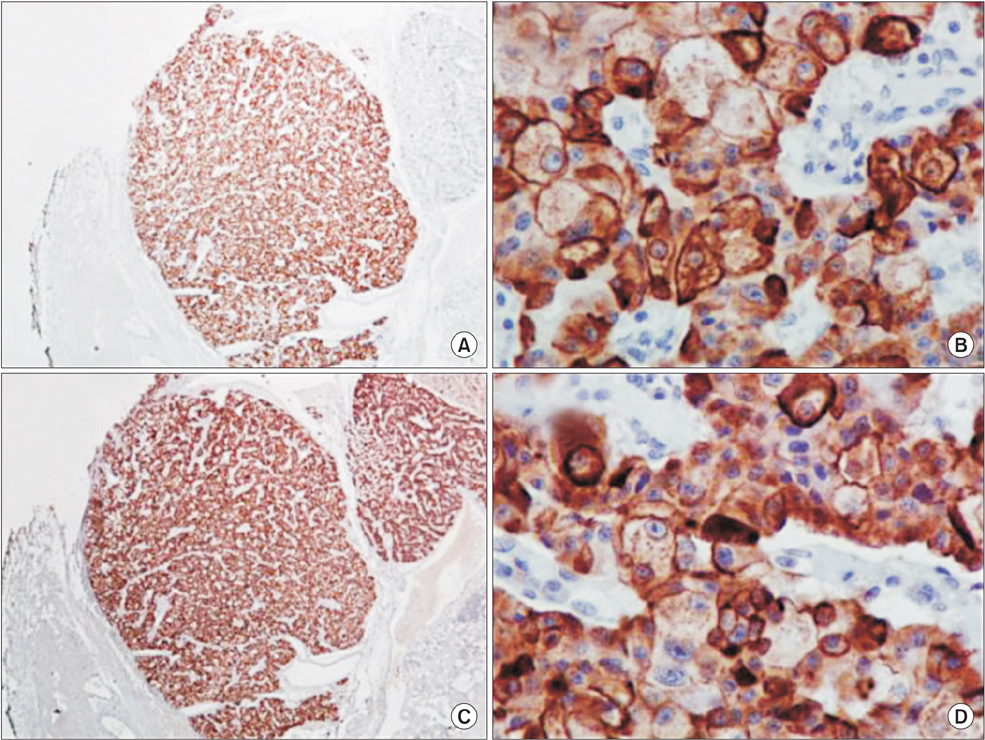
Fig. 5 (A, B) Immunohistochemical expression of cytokeratin E1 from tumor cells. Streptavidin-biotin peroxidase (A, ×100; B, ×400). (C, D) Immunohistochemical expression of cytokeratin E3 from tumor cells. Streptavidin-biotin peroxidase (A, ×100; B, ×400).

Fig. 6 (A, B) Immunohistochemical expression of polyclonal CEA from tumor cells. Streptavidin-biotin peroxidase (A, ×100; B, ×400). (C, D) Immunohistochemical expression of insulin from tumor cells. Streptavidin-biotin peroxidase (A, ×100; B, ×400).
Reference
-
1. Service FJ, McMahon MM, O'Brien PC, Ballard DJ. Functioning insulinoma--incidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clin Proc. 1991; 66:711–719.2. Kulke MH, Anthony LB, Bushnell DL, de Herder WW, Goldsmith SJ, Klimstra DS, et al. Tumor Society (NANETS). NANETS treatment guidelines: well-differentiated neuroendocrine tumors of the stomach and pancreas. Pancreas. 2010; 39:735–752.3. Mansour JC, Chen H. Pancreatic endocrine tumors. J Surg Res. 2004; 120:139–161.4. Whipple AO, Frantz VK. Adenoma of islet cells with hyperinsulinism: a review. Ann Surg. 1935; 101:1299–1335.5. Vinik AI, Woltering EA, Warner RR, Caplin M, O'Dorisio TM, Wiseman GA, et al. NANETS consensus guidelines for the diagnosis of neuroendocrine tumor. Pancreas. 2010; 39:713–734.6. Alexakis N, Neoptolemos JP. Pancreatic neuroendocrine tumours. Best Pract Res Clin Gastroenterol. 2008; 22:183–205.7. Balon HR, Goldsmith SJ, Siegel BA, Silberstein EB, Krenning EP, Lang O, et al. Procedure guideline for somatostatin receptor scintigraphy with (111)In-pentetreotide. J Nucl Med. 2001; 42:1134–1138.8. Tucker ON, Crotty PL, Conlon KC. The management of insulinoma. Br J Surg. 2006; 93:264–275.9. Oberg K. Pancreatic endocrine tumors. Semin Oncol. 2010; 37:594–618.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Malignant Insulinoma Resistant to Octreotide and Combination Chemotherapy
- Successful Endoscopic Ultrasound-Guided Alcohol Ablation of Sporadic Insulinoma Using Three-Dimensional Targeting (with Video)
- Clinical Significance of Hyperinsulinsism - Diagnosis of Insulinoma
- A Case of Insulinoma without Peripheral Hyperinsulinemia
- Malignant Giant Cell Tumor of the Skull
