Palliative Radiotherapy in a Patient with Pulmonary Adenoid Cystic Carcinoma
- Affiliations
-
- 1Department of Radiation Oncology, Dankook University College of Medicine, Cheonan, Korea. merdeglas@dankook.ac.kr
Abstract
- Primary adenoid cystic carcinoma in the lung is very rare, so its clinicopathologic characteristics have usually been extrapolated from the salivary disease. However, the clinical courses of pulmonary adenoid cystic carcinomas may be different from those of salivary disease, and individual differences may also exist. I report here on a case of a patient who was initially diagnosed as pulmonary adenoid cystic carcinoma with liver metastases and the tumor showed extreme radiosensitivity, but it also underwent an aggressive clinical course. Adenoid cystic carcinoma is usually known to be a slowly growing tumor, but it may rapidly disseminate, like in this patient. Therefore, the factors predicting aggressive behavior should be determined and the treatment might be individualized according to the primary sites and on the patient's basis.
MeSH Terms
Figure
-
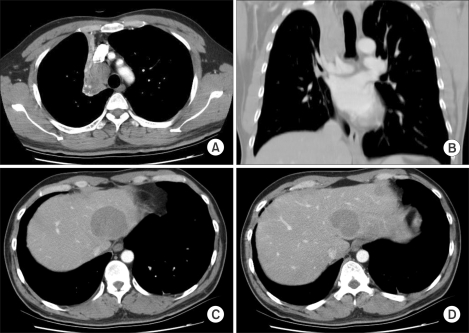
Fig. 1 Initial CT findings. (A, B) On chest CT, a mass obstructing the right upper lobar bronchus was detected and it caused atelectasis of the right upper lobe. A 2.5 cm sized lymph node was also detected at the right paratracheal nodal station. (C, D) Multiple hepatic metastases were detected at the time of the initial diagnosis.
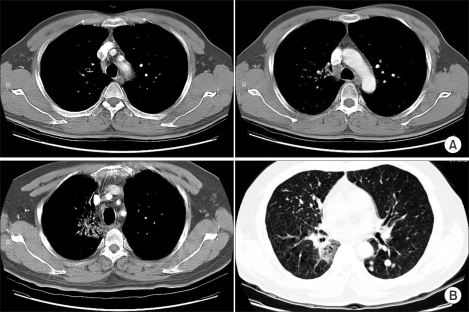
Fig. 2 Chest CT findings after thoracic radiotherapy. (A) Immediate post-radiotherapy. The chest CT scan, which was performed 2 weeks after radiotherapy, showed a markedly decreased RUL mass and right lower paratracheal lymph node (<1 cm). (B) 9 months after thoracic radiotherapy. There was no evidence of disease recurrence at the previously irradiated sites, with only asymptomatic radiation pneumonitis being seen. There were multiple, newly detected pulmonary metastases.
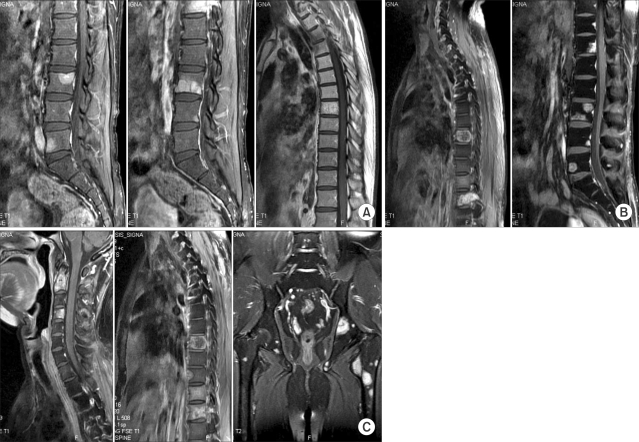
Fig. 3 Rapidly progressing multiple bone metastases. (A) 1 month after thoracic radiotherapy. (B) 4 months after thoracic radiotherapy. (C) 6 months after thoracic radiotherapy. Bone metastases were initially diagnosed at 1 month after thoracic irradiation and then these lesions rapidly progressed. After 6.5 months, the bone metastases had progressed to the whole spine, except for the previously irradiated upper thoracic spine, and the progression also involved the pelvis, femur and sternum.
Reference
-
1. Nomori H, Kaseda S, Kobayashi K, Ishihara T, Yanai N, Torikata C. Adenoid cystic carcinoma of the trachea and main-stem bronchus. A clinical, histopathologic, and immunohistochemical study. J Thorac Cardiovasc Surg. 1988; 96:271–277. PMID: 2456426.2. Moran CA, Suster S, Koss MN. Primary adenoid cystic carcinoma of the lung. A clinicopathologic and immunohistochemistry study of 16 cases. Cancer. 1994; 73:1390–1397. PMID: 7509254.3. Lawrence JB, Mazur MT. Adenoid cystic carcinoma: a comparative pathologic study of tumors in salivary gland, breast, lung and cervix. Hum Pathol. 1982; 13:916–924. PMID: 6290368.
Article4. Sweeney WB, Thomas JM. Adenoid cystic carcinoma of the lung. Contemp Surg. 1986; 28:97–100.5. Shin SJ, Rosen PP. Solid variant of mammary adenoid cystic carcinoma with basaloid features: a study of nine cases. Am J Surg Pathol. 2002; 26:413–420. PMID: 11914618.6. Cerar A, Jutersek A, Vidmar S. Adenoid cystic carcinoma of the esophagus. A clinicopathologic study of three cases. Cancer. 1991; 67:2159–2164. PMID: 1706215.
Article7. Kanematsu T, Yohena T, Uehara T, Ushijima C, Asoh H, Yoshino I, et al. Treatment outcome of resected and nonresected primary adenoid cystic carcinoma of the lung. Ann Thorac Cardiovasc Surg. 2002; 8:74–77. PMID: 12027791.8. Gaissert HA, Grillo HC, Shadmehr M, Wright CD, Gokhale M, Wain JC, et al. Long-term survival after resection of primary adenoid cystic and squamous cell carcinoma of the trachea and carina. Ann Thorac Surg. 2004; 78:1889–1897. PMID: 15560996.
Article9. Weber AL, Grillo HC. Tracheal tumors: a radiological, clinical and pathological evaluation of 84 cases. Radiol Clin North Am. 1978; 16:227–246. PMID: 212775.10. Albers E, Lawrie T, Harrell JH, Yi ES. Tracheobroncheal adenoid cystic carcinoma: A clinicopathologic study of 14 cases. Chest. 2004; 125:1160–1165. PMID: 15006985.11. Spiro RH, Huvos AG. Stage means more than grade in adenoid cystic carcinoma. Am J Surg. 1992; 164:623–628. PMID: 1334380.
Article12. Sung MW, Kim KH, Kim JW, Min YG, Seong WJ, Roh JL, et al. Clinicopathological predictors and impact of distant metastasis from adenoid cystic carcinoma of the head and neck. Arch Otolaryngol Head Neck Surg. 2003; 129:1193–1197. PMID: 14623749.13. Pastolero G, Hanna W, Zbieranowski I, Kahn HJ. Proliferative activity and p53 expression in adenoid cystic carcinoma of the breast. Mod Pathol. 1996; 9:215–219. PMID: 8685217.14. van der Wal JE, Becking AG, Show GB, van der Wal I. Distant metastases of adenoid cystic carcinoma of the salivary glands and the value of diagnostic examinations during follow-up. Head Neck. 2002; 24:779–783. PMID: 12203804.
Article15. Lin CM, Li AF, Wu LH, Wu YC, Lin FC, Wang LS. Aednoid cystic carcinoma of the trachea and bronchus- a clinicopathologic study with DNA flow cytometric analysis and oncogene expression. Eur J Cardiothorac Surg. 2002; 22:621–625. PMID: 12297183.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Adenoid Cystic Carcinoma of the Bartholin's Gland
- A case of adenoid basal cell carcinoma in uterine cervix
- Adenoid Basal Carcinoma and Adenoid Cystic Carcinoma of the Uterine Cervix: A Study of 2 Cases
- A Case of Adenoid Cystic Carcinoma on Subglottis
- Dedifferentiation in Adenoid Cystic Carcinoma of the Neck
