Functional Electrical Stimulation to Ankle Dorsiflexor and Plantarflexor Using Single Foot Switch in Patients With Hemiplegia From Hemorrhagic Stroke
- Affiliations
-
- 1Department of Rehabilitation Medicine, Wonju Severance Christian Hospital, Yonsei University College of Medicine, Wonju, Korea. enmcse@hanmail.net
- 2Department of Biomedical Engineering, Institute of Medical Engineering, Yonsei University, Wonju, Korea.
- 3Department of Rehabilitation Science and Technology, University of Pittsburgh, PA, USA.
- KMID: 2165747
- DOI: http://doi.org/10.5535/arm.2014.38.3.310
Abstract
OBJECTIVE
To evaluate the effects of functional electrical stimulation (FES) to ankle dorsiflexor (DF) and ankle plantarflexor (PF) on kinematic and kinetic parameters of hemiplegic gait.
METHODS
Fourteen post-stroke hemiplegic patients were considered in this study. Electrical stimulation was delivered to ankle DF during the swing phase and ankle PF during the stance phase via single foot switch. Kinematic and kinetic data were collected using a computerized motion analysis system with force plate. Data of no stimulation (NS), DF stimulation only (DS), DF and PF stimulation (DPS) group were compared among each other.
RESULTS
Peak ankle dorsiflexion angle during swing phase is significantly greater in DS group (-1.55degrees+/-9.10degrees) and DPS group (-2.23degrees+/-9.64degrees), compared with NS group (-6.71degrees+/-11.73degrees) (p<0.05), although there was no statistically significant difference between DS and DPS groups. Ankle plantarflexion angle at toe-off did not show significant differences among NS, DS, and DPS groups. Peak knee flexion in DPS group (34.12degrees+/-13.77degrees) during swing phase was significantly greater than that of NS group (30.78degrees+/-13.64degrees), or DS group (32.83degrees+/-13.07degrees) (p<0.05).
CONCLUSION
In addition to the usual FES application stimulating ankle DF during the swing phase, stimulation of ankle PF during stance phase can help to increase peak knee flexion during the swing phase. This study shows the advantages of stimulating the ankle DF and PF using single foot switch for post-stroke gait.
Keyword
MeSH Terms
Figure
-
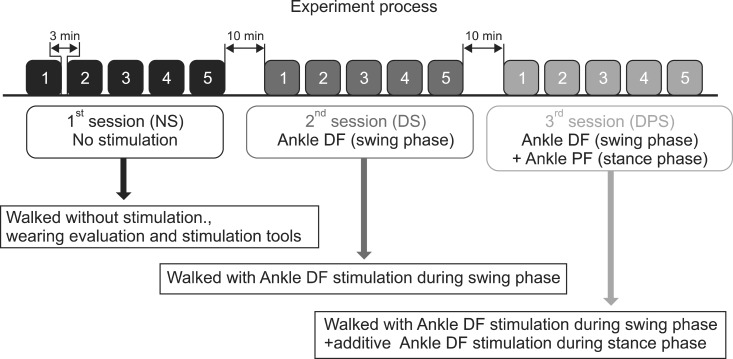
Fig. 1 Performed total of three test sessions: 1) patient was asked to ambulate on test way without any stimulation (NS); 2) patient ambulated with ankle DF stimulation during the swing phase (DS), 3) patient ambulated with additive ankle PF stimulation during the stance phase (DPS), which is composed of 5 trials each, these were performed with 10-minute intersession break and a 3-minute inter-trial break to avoid fatigue. DF, dorsiflexor; PF, plantarflexor; NS, no stimulation; DS, DF stimulation only; DPS, DF and PF stimulation.
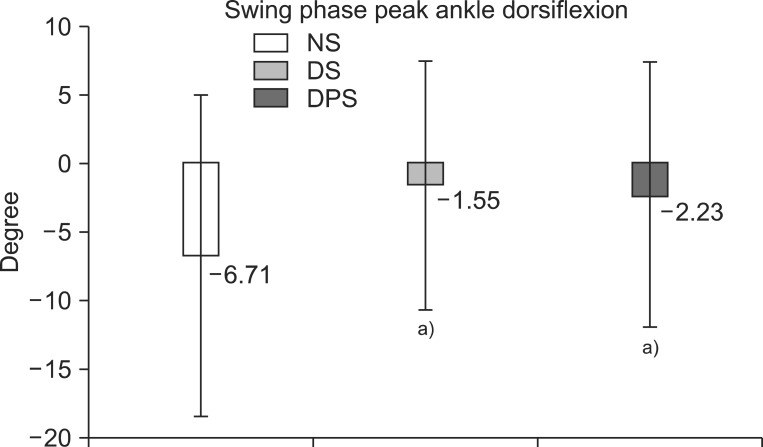
Fig. 2 Swing phase peak ankle dorsiflexion angle was significantly greater in dorsiflexor stimulation only group (DS, -1.55°±9.10°) and dorsiflexor and plantarflexor stimulation group (DPS, -2.23°±9.64°), compared with no stimulation group (NS, -6.71°±11.73°) (p<0.05), although there was no statistically significant difference between DS and DPS groups. a)p<0.05, significant difference from no stimulation.
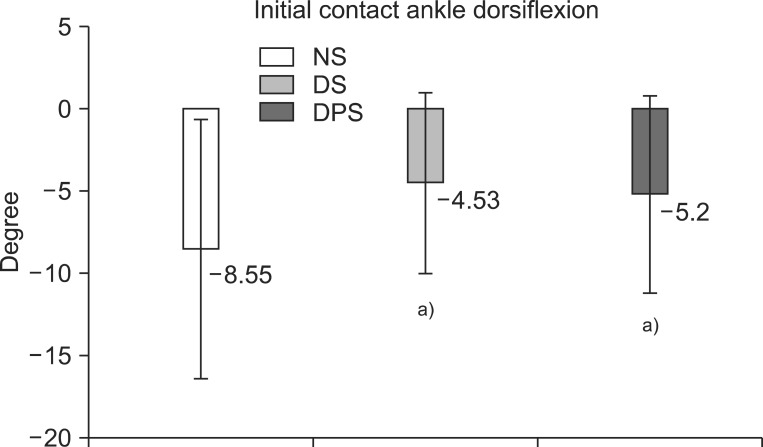
Fig. 3 Initial contact ankle dorsiflexion angle was still significantly greater continuing to swing phase (Fig. 2) in dorsiflexor stimulation only group (DS, -4.53°±2.73°) and dorsiflexor and plantarflexor stimulation group (DPS, -5.20°±3.01°), compared with no stimulation group (NS, -8.55°±3.93°). a)p<0.05, significant difference from no stimulation.
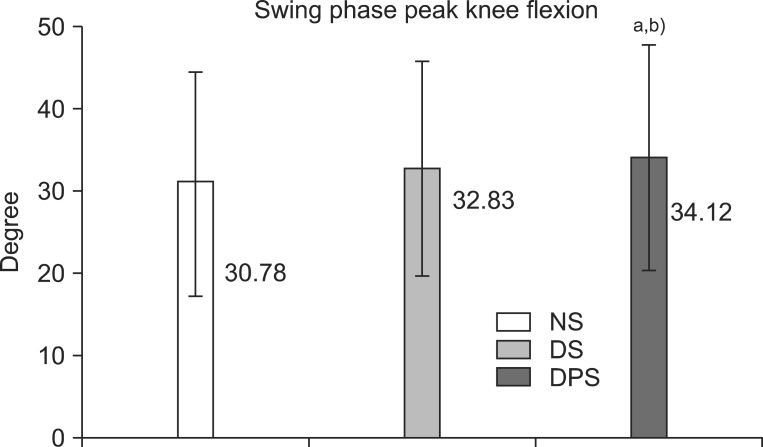
Fig. 4 Swing phase peak knee flexion was significantly greater in order of dorsiflexor and plantarflexor stimulation group (DPS, 34.12°±13.77°), dorsiflexor stimulation only group (DS, 32.83°±13.07°), and no stimulation group (NS, 30.78°±13.64°). a)p<0.05, significant difference from no stimulation. b)p<0.05, significant difference from dorsiflexor stimulation only.
Reference
-
1. Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet. 2011; 377:1693–1702. PMID: 21571152.
Article2. Dickstein R. Rehabilitation of gait speed after stroke: a critical review of intervention approaches. Neurorehabil Neural Repair. 2008; 22:649–660. PMID: 18971380.
Article3. Stein RB, Chong S, Everaert DG, Rolf R, Thompson AK, Whittaker M, et al. A multicenter trial of a footdrop stimulator controlled by a tilt sensor. Neurorehabil Neural Repair. 2006; 20:371–379. PMID: 16885423.
Article4. Taylor PN, Burridge JH, Dunkerley AL, Wood DE, Norton JA, Singleton C, et al. Clinical use of the Odstock dropped foot stimulator: its effect on the speed and effort of walking. Arch Phys Med Rehabil. 1999; 80:1577–1583. PMID: 10597809.
Article5. Neptune RR, Kautz SA, Zajac FE. Contributions of the individual ankle plantar flexors to support, forward progression and swing initiation during walking. J Biomech. 2001; 34:1387–1398. PMID: 11672713.
Article6. Anderson FC, Goldberg SR, Pandy MG, Delp SL. Contributions of muscle forces and toe-off kinematics to peak knee flexion during the swing phase of normal gait: an induced position analysis. J Biomech. 2004; 37:731–737. PMID: 15047002.
Article7. Kesar TM, Perumal R, Reisman DS, Jancosko A, Rudolph KS, Higginson JS, et al. Functional electrical stimulation of ankle plantarflexor and dorsiflexor muscles: effects on poststroke gait. Stroke. 2009; 40:3821–3827. PMID: 19834018.8. Embrey DG, Holtz SL, Alon G, Brandsma BA, McCoy SW. Functional electrical stimulation to dorsiflexors and plantar flexors during gait to improve walking in adults with chronic hemiplegia. Arch Phys Med Rehabil. 2010; 91:687–696. PMID: 20434604.
Article9. Teixeira-Salmela LF, Nadeau S, Mcbride I, Olney SJ. Effects of muscle strengthening and physical conditioning training on temporal, kinematic and kinetic variables during gait in chronic stroke survivors. J Rehabil Med. 2001; 33:53–60. PMID: 11474950.10. Kerrigan DC, Karvosky ME, Riley PO. Spastic paretic stiff-legged gait: joint kinetics. Am J Phys Med Rehabil. 2001; 80:244–249. PMID: 11277129.11. Nadeau S, Gravel D, Arsenault AB, Bourbonnais D. Plantarflexor weakness as a limiting factor of gait speed in stroke subjects and the compensating role of hip flexors. Clin Biomech (Bristol, Avon). 1999; 14:125–135.
Article12. Jonkers I, Delp S, Patten C. Capacity to increase walking speed is limited by impaired hip and ankle power generation in lower functioning persons post-stroke. Gait Posture. 2009; 29:129–137. PMID: 18789692.
Article13. Kesar TM, Perumal R, Jancosko A, Reisman DS, Rudolph KS, Higginson JS, et al. Novel patterns of functional electrical stimulation have an immediate effect on dorsiflexor muscle function during gait for people poststroke. Phys Ther. 2010; 90:55–66. PMID: 19926681.
Article14. Chen CL, Chen HC, Tang SF, Wu CY, Cheng PT, Hong WH. Gait performance with compensatory adaptations in stroke patients with different degrees of motor recovery. Am J Phys Med Rehabil. 2003; 82:925–935. PMID: 14627929.
Article15. Chen G, Patten C, Kothari DH, Zajac FE. Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds. Gait Posture. 2005; 22:51–56. PMID: 15996592.
Article16. Olney SJ, Richards C. Hemiparetic gait following stroke, Part I: characteristics. Gait Posture. 1996; 4:136–148.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Electrical Stimulation on Spasticity in Hemiplegic Patients
- Effect of Plastic Ankle Foot Orthosis and Functional Electrical Stimulation on Hemiplegic Gait
- Comprehensive Rehabilitation in Patients with Acute Respiratory Distress Syndrome due to Coronavirus Disease 2019 (COVID-19)
- Rehabilitation after Surgical Repair of the Achilles Tendon Rupture : Cases report
- Comparison of the Electromyographic Activity of the Tibialis Anterior and Isometric Dorsiflexor Strength during Dorsiflexion According to Toe Postures in Individuals with Ankle Dorsiflexor Weakness
