Effect of Constraint-Induced Movement Therapy and Mirror Therapy for Patients With Subacute Stroke
- Affiliations
-
- 1Department of Rehabilitation Medicine, Pusan National University School of Medicine, Busan, Korea. rmshin01@gmail.com
- KMID: 2165728
- DOI: http://doi.org/10.5535/arm.2014.38.4.458
Abstract
OBJECTIVE
To evaluate the effectiveness of constraint-induced movement therapy (CIMT) and combined mirror therapy for inpatient rehabilitation of the patients with subacute stroke.
METHODS
Twenty-six patients with subacute stroke were enrolled and randomly divided into three groups: CIMT combined with mirror therapy group, CIMT only group, and control group. Two weeks of CIMT for 6 hours a day with or without mirror therapy for 30 minutes a day were performed under supervision. All groups received conventional occupational therapy for 40 minutes a day for the same period. The CIMT only group and control group also received additional self-exercise to substitute for mirror therapy. The box and block test, 9-hole Pegboard test, grip strength, Brunnstrom stage, Wolf motor function test, Fugl-Meyer assessment, and the Korean version of Modified Barthel Index were performed prior to and two weeks after the treatment.
RESULTS
After two weeks of treatment, the CIMT groups with and without mirror therapy showed higher improvement (p<0.05) than the control group, in most of functional assessments for hemiplegic upper extremity. The CIMT combined with mirror therapy group showed higher improvement than CIMT only group in box and block test, 9-hole Pegboard test, and grip strength, which represent fine motor functions of the upper extremity.
CONCLUSION
The short-term CIMT combined with mirror therapy group showed more improvement compared to CIMT only group and control group, in the fine motor functions of hemiplegic upper extremity for the patients with subacute stroke.
Keyword
MeSH Terms
Figure
-

Fig. 1 Flow diagram of this study.
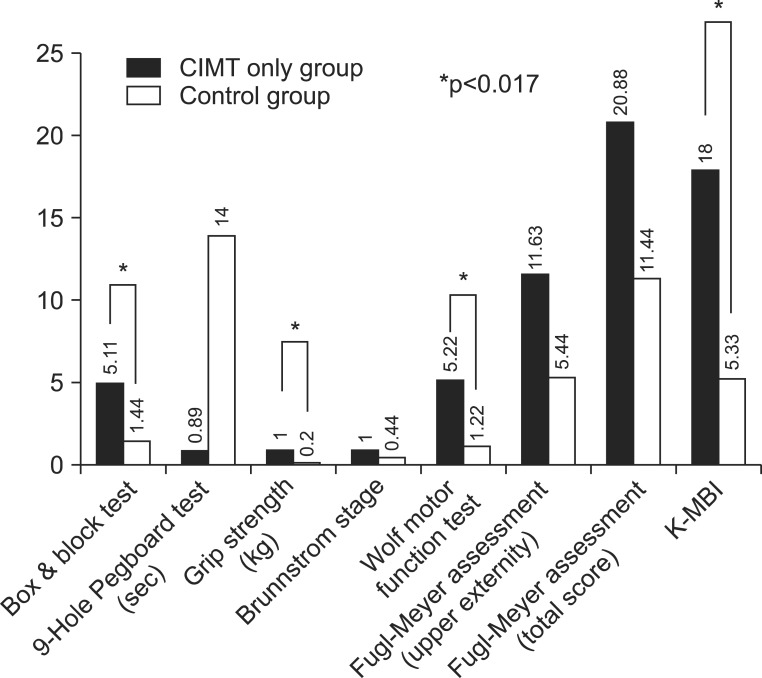
Fig. 2 Difference in percentage of assessment at baseline and after treatment in CIMT only group vs. control group (*p<0.017). CIMT, constraint-induced movement therapy; K-MBI, Korean version of Modified Barthel Index.

Fig. 3 Difference in percentage of assessment at baseline and after treatment in CIMT with mirror therapy group vs. control group (*p<0.017). CIMT, constraint-induced movement therapy; K-MBI, Korean version of Modified Barthel Index.

Fig. 4 Difference in percentage of assessment at baseline and after treatment in CIMT with mirror therapy group vs. CIMT only group (*p<0.017). CIMT, constraint-induced movement therapy; K-MBI, Korean version of Modified Barthel Index.
Cited by 2 articles
-
Efficacy of Mirror Therapy Containing Functional Tasks in Poststroke Patients
Kil-Byung Lim, Hong-Jae Lee, Jeehyun Yoo, Hyun-Ju Yun, Hye-Jung Hwang
Ann Rehabil Med. 2016;40(4):629-636. doi: 10.5535/arm.2016.40.4.629.Can Short-Term Constraint-Induced Movement Therapy Combined With Visual Biofeedback Training Improve Hemiplegic Upper Limb Function of Subacute Stroke Patients?
Hyun Seok, Seung Yeol Lee, Jihoon Kim, Jungho Yeo, Hyungdong Kang
Ann Rehabil Med. 2016;40(6):998-1009. doi: 10.5535/arm.2016.40.6.998.
Reference
-
1. Basmajian JV. The Winter of Our Discontent: breaking intolerable time locks for stroke survivors. The 38th annual John Stanley Coulter lecture. Arch Phys Med Rehabil. 1989; 70:92–94. PMID: 2916934.2. Pang MY, Harris JE, Eng JJ. A community-based upper-extremity group exercise program improves motor function and performance of functional activities in chronic stroke: a randomized controlled trial. Arch Phys Med Rehabil. 2006; 87:1–9. PMID: 16401430.
Article3. Taub E, Miller NE, Novack TA, Cook EW 3rd, Fleming WC, Nepomuceno CS, et al. Technique to improve chronic motor deficit after stroke. Arch Phys Med Rehabil. 1993; 74:347–354. PMID: 8466415.4. Taub E, Wolf SL. Constraint induced movement techniques to facilitate upper extremity use in stroke patients. Top Stroke Rehabil. 1997; 3:38–61.
Article5. Dromerick AW, Edwards DF, Hahn M. Does the application of constraint-induced movement therapy during acute rehabilitation reduce arm impairment after ischemic stroke? Stroke. 2000; 31:2984–2988. PMID: 11108760.
Article6. Page SJ, Sisto S, Johnston MV, Levine P, Hughes M. Modified constraint-induced therapy in subacute stroke: a case report. Arch Phys Med Rehabil. 2002; 83:286–290. PMID: 11833037.
Article7. Peurala SH, Kantanen MP, Sjogren T, Paltamaa J, Karhula M, Heinonen A. Effectiveness of constraint-induced movement therapy on activity and participation after stroke: a systematic review and meta-analysis of randomized controlled trials. Clin Rehabil. 2012; 26:209–223. PMID: 22070990.
Article8. Ramachandran VS, Rogers-Ramachandran D. Synaesthesia in phantom limbs induced with mirrors. Proc Biol Sci. 1996; 263:377–386. PMID: 8637922.9. Altschuler EL, Wisdom SB, Stone L, Foster C, Galasko D, Llewellyn DM, et al. Rehabilitation of hemiparesis after stroke with a mirror. Lancet. 1999; 353:2035–2036. PMID: 10376620.
Article10. Bonifer NM, Anderson KM, Arciniegas DB. Constraint-induced movement therapy after stroke: efficacy for patients with minimal upper-extremity motor ability. Arch Phys Med Rehabil. 2005; 86:1867–1873. PMID: 16181956.
Article11. Taub E. Somatosensory deafferentation research with monkeys: implications for rehabilitation medicine. In : Ince LP, editor. Behavioral psychology in rehabilitation medicine: clinical applications. New York: Williams & Wilkins;1980. p. 371–401.12. Taub E. Movement in nonhuman primates deprived of somatosensory feedback. Exerc Sport Sci Rev. 1976; 4:335–374. PMID: 828579.13. Wilkinson PR, Wolfe CD, Warburton FG, Rudd AG, Howard RS, Ross-Russell RW, et al. A long-term follow-up of stroke patients. Stroke. 1997; 28:507–512. PMID: 9056603.
Article14. Schaechter JD, Moore CI, Connell BD, Rosen BR, Dijkhuizen RM. Structural and functional plasticity in the somatosensory cortex of chronic stroke patients. Brain. 2006; 129(Pt 10):2722–2733. PMID: 16921177.
Article15. Dancause N, Barbay S, Frost SB, Plautz EJ, Chen D, Zoubina EV, et al. Extensive cortical rewiring after brain injury. J Neurosci. 2005; 25:10167–10179. PMID: 16267224.
Article16. Gauthier LV, Taub E, Perkins C, Ortmann M, Mark VW, Uswatte G. Remodeling the brain: plastic structural brain changes produced by different motor therapies after stroke. Stroke. 2008; 39:1520–1525. PMID: 18323492.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of Mirror Therapy on the Balance, Gait and Motor Function in Patients with Subacute Stroke
- Effect of Mirror Therapy on Recovery of Upper Limb Function and Strength in Subacute Hemiplegia after Stroke
- Efficacy of Mirror Therapy Containing Functional Tasks in Poststroke Patients
- Can Short-Term Constraint-Induced Movement Therapy Combined With Visual Biofeedback Training Improve Hemiplegic Upper Limb Function of Subacute Stroke Patients?
- The Effect of Modified Constraint-induced Movement Therapy for the Stroke Patients in Inpatient Setting
