Clin Endosc.
2016 May;49(3):282-288. 10.5946/ce.2015.046.
Optimal Methods for the Management of Iatrogenic Colonoscopic Perforation
- Affiliations
-
- 1Department of Internal Medicine, CHA Bundang Medical Center, CHA University, Seongnam, Korea. sphong@cha.ac.kr
- 2Department of Surgery, CHA Bundang Medical Center, CHA University, Seongnam, Korea.
- KMID: 2165023
- DOI: http://doi.org/10.5946/ce.2015.046
Abstract
- BACKGROUND/AIMS
Colonoscopic perforations have been managed with exploratory laparotomy, and have resulted in some morbidity and mortality. Recently, laparoscopic surgery is commonly performed for this purpose. The aim of this study was to compare the outcomes of several management strategies for iatrogenic colonoscopic perforations.
METHODS
We retrospectively reviewed the medical records of patients who had been treated for colonoscopic perforation between January 2004 and April 2013 at CHA Bundang Medical Center in Korea.
RESULTS
A total of 41 patients with colonoscopic perforation were enrolled. Twenty patients underwent conservative management with a success rate of 90%. Surgical management was performed in 23 patients including two patients who were converted to surgical management after the failure of the initial conservative management. Among 14 patients who underwent surgery at 8 hours after the perforation, there was no considerable difference in adverse outcomes between the laparotomy group and the laparoscopic surgery group. The medical costs and claim rate were 1.45 and 1.87 times greater in the exploratory laparotomy group, respectively.
CONCLUSIONS
Conservative management of colonoscopic perforation could be an option for patients without overt symptoms of peritonitis or with a small defect size. If surgical management is required, laparoscopic surgery may be considered as the initial procedure even with a delayed diagnosis.
MeSH Terms
Figure
-
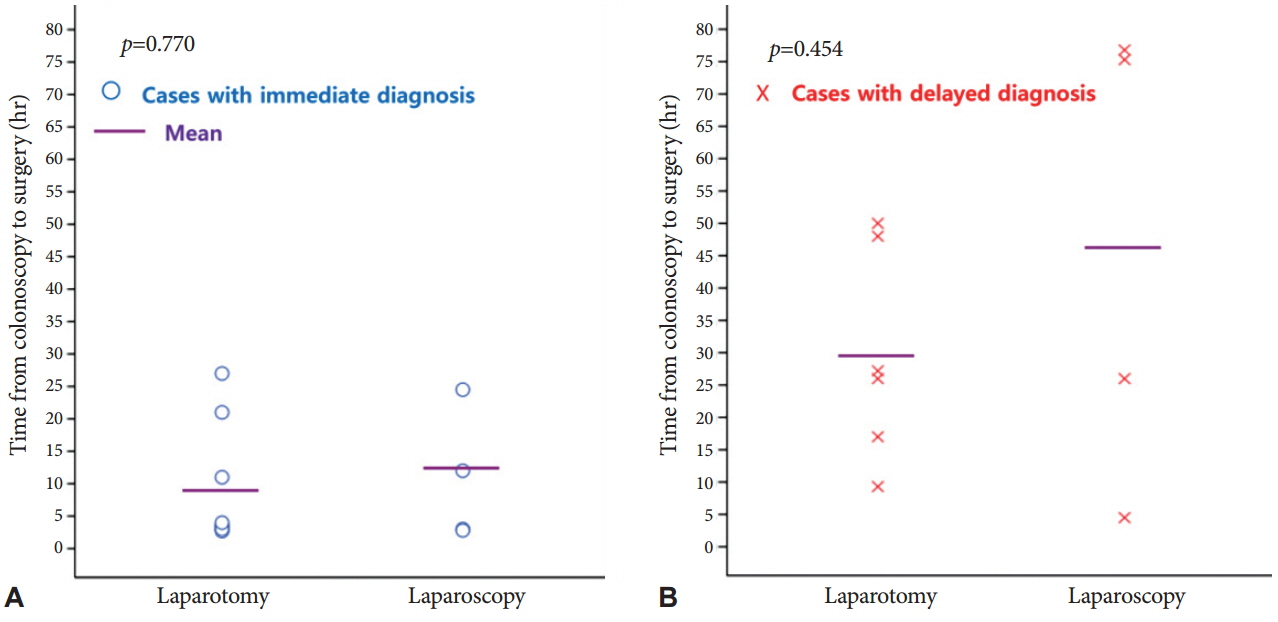
Fig. 1. Elapsed time from perforation to surgery according to the awareness of the perforation. (A) Elapsed time in patients with an immediate diagnosis of perforation. (B) Elapsed time in patients with a delayed diagnosis of perforation. There was no statistical difference in the elapsed time between laparotomy and laparoscopy.

Fig. 2. Flow chart for the management of iatrogenic colonoscopic perforation. Colonoscopic perforations could be found during or after procedures. This figure shows processes and clinical outcomes of each management for colonoscopic perforations.
Cited by 1 articles
-
How Should We Manage Iatrogenic Perforation Caused by Colonoscopy?
Eun Sun Kim
Clin Endosc. 2016;49(3):214-215. doi: 10.5946/ce.2016.072.
Reference
-
1. Kim JS, Kim BW, Kim JI, et al. Endoscopic clip closure versus surgery for the treatment of iatrogenic colon perforations developed during diagnostic colonoscopy: a review of 115,285 patients. Surg Endosc. 2013; 27:501–504.
Article2. Namgung H, Cho MK, Lee KH, et al. Management of colonic perforation during colonoscopic procedure. Korean J Gastrointest Endosc. 2005; 30:188–193.3. Hall C, Dorricott NJ, Donovan IA, Neoptolemos JP. Colon perforation during colonoscopy: surgical versus conservative management. Br J Surg. 1991; 78:542–544.
Article4. Lo AY, Beaton HL. Selective management of colonoscopic perforations. J Am Coll Surg. 1994; 179:333–337.5. Jentschura D, Raute M, Winter J, Henkel T, Kraus M, Manegold BC. Complications in endoscopy of the lower gastrointestinal tract: therapy and prognosis. Surg Endosc. 1994; 8:672–676.6. Kavic SM, Basson MD. Complications of endoscopy. Am J Surg. 2001; 181:319–332.
Article7. Iqbal CW, Cullinane DC, Schiller HJ, Sawyer MD, Zietlow SP, Farley DR. Surgical management and outcomes of 165 colonoscopic perforations from a single institution. Arch Surg. 2008; 143:701–706.
Article8. Arora G, Mannalithara A, Singh G, Gerson LB, Triadafilopoulos G. Risk of perforation from a colonoscopy in adults: a large population-based study. Gastrointest Endosc. 2009; 69(3 Pt 2):654–664.
Article9. La Torre M, Velluti F, Giuliani G, Di Giulio E, Ziparo V, La Torre F. Promptness of diagnosis is the main prognostic factor after colonoscopic perforation. Colorectal Dis. 2012; 14:e23–e26.
Article10. Matharoo GS, Goldfarb MA. Treatment and outcomes of iatrogenic colon perforations at a community teaching hospital. Am Surg. 2012; 78:975–978.
Article11. Na EJ, Kim KJ, Min YD. Safety of conservative treatment of colonoscopic perforation. J Korean Soc Coloproctol. 2005; 21:384–389.12. Magdeburg R, Collet P, Post S, Kaehler G. Endoclipping of iatrogenic colonic perforation to avoid surgery. Surg Endosc. 2008; 22:1500–1504.
Article13. Coimbra C, Bouffioux L, Kohnen L, et al. Laparoscopic repair of colonoscopic perforation: a new standard? Surg Endosc. 2011; 25:1514–1517.
Article14. Bleier JI, Moon V, Feingold D, et al. Initial repair of iatrogenic colon perforation using laparoscopic methods. Surg Endosc. 2008; 22:646–649.
Article15. Miranda L, Settembre A, Piccolboni D, Capasso P, Corcione F. Iatrogenic colonic perforation: repair using laparoscopic technique. Surg Laparosc Endosc Percutan Tech. 2011; 21:170–174.16. Makarawo TP, Damadi A, Mittal VK, Itawi E, Rana G. Colonoscopic perforation management by laparoendoscopy: an algorithm. JSLS. 2014; 18:20–27.
Article17. Christie JP, Marrazzo J 3rd. “Mini-perforation” of the colon: not all postpolypectomy perforations require laparotomy. Dis Colon Rectum. 1991; 34:132–135.18. Cho YK, Nam SW, Kim HC, et al. Conservative treatment of colonoscopic perforations. Korean J Gastrointest Endosc. 2006; 33:20–25.19. Castellví J, Pi F, Sueiras A, et al. Colonoscopic perforation: useful parameters for early diagnosis and conservative treatment. Int J Colorectal Dis. 2011; 26:1183–1190.
Article20. Raju GS, Saito Y, Matsuda T, Kaltenbach T, Soetikno R. Endoscopic management of colonoscopic perforations (with videos). Gastrointest Endosc. 2011; 74:1380–1388.
Article21. Wu J, Hu B. The role of carbon dioxide insufflation in colonoscopy: a systematic review and meta-analysis. Endoscopy. 2012; 44:128–136.
Article22. Vincent M, Smith LE. Management of perforation due to colonoscopy. Dis Colon Rectum. 1983; 26:61–63.
Article23. Magdeburg R, Sold M, Post S, Kaehler G. Differences in the endoscopic closure of colonic perforation due to diagnostic or therapeutic colonoscopy. Scand J Gastroenterol. 2013; 48:862–867.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Colonoscopic Perforation; A 10-year Experience in Single General Hospital
- Colonoscopic Perforations: 4 Years' Experience
- Recurrent Colonic Perforation after Successful Conservative Treatment of Colonoscopic Perforation
- The Iatrogenic Complications of Colonoscopic Polypectomy: A Multicenter Retrospective Study
- Pneumothorax, Pneumomediastinum, Subcutaneous Emphysema, Pneumoretroperitoneum Secondary to Colonoscopic Perforation
