CT Quantification of Central Airway in Tracheobronchomalacia
- Affiliations
-
- 1Department of Radiology, Chonbuk National University Hospital, Jeonju, Korea. gyjin@jbnu.ac.kr
- 2Department of Radiology, Chonbuk National University School of Medicine, Jeonju, Korea.
- 3Research Institute of Clinical Medicine of Chonbuk National University-Biomedical Research Institute of Chonbuk National University Hospital, Jeonju, Korea.
- KMID: 2164825
- DOI: http://doi.org/10.3348/jksr.2016.74.5.299
Abstract
- PURPOSE
To know which factors help to diagnose tracheobronchomalacia (TBM) using CT quantification of central airway.
MATERIALS AND METHODS
From April 2013 to July 2014, 19 patients (68.0 ± 15.0 years; 6 male, 13 female) were diagnosed as TBM on CT. As case-matching, 38 normal subjects (65.5 ± 21.5 years; 6 male, 13 female) were selected. All 57 subjects underwent CT with end-inspiration and end-expiration. Airway parameters of trachea and both main bronchus were assessed using software (VIDA diagnostic). Airway parameters of TBM patients and normal subjects were compared using the Student t-test.
RESULTS
In expiration, both wall perimeter and wall thickness in TBM patients were significantly smaller than normal subjects (wall perimeter: trachea, 43.97 mm vs. 49.04 mm, p = 0.020; right main bronchus, 33.52 mm vs. 42.69 mm, p < 0.001; left main bronchus, 26.76 mm vs. 31.88 mm, p = 0.012; wall thickness: trachea, 1.89 mm vs. 2.22 mm, p = 0.017; right main bronchus, 1.64 mm vs. 1.83 mm, p = 0.021; left main bronchus, 1.61 mm vs. 1.75 mm, p = 0.016).
CONCLUSION
Wall thinning and decreased perimeter of central airway of expiration by CT quantification would be a new diagnostic indicators in TBM.
MeSH Terms
Figure
-

Fig. 1 CT (axial plane) and three-dimensional reconstructed VIDA images (axial and coronal view) of normal and tracheobronchomalacia group. Inspiration (A) and expiration (B) of normal subjects: there is no significant change of tracheal luminal area on inspiration and expiration. Inspiration (C) and expiration (D) of tracheobronchomalacia patients: the luminal area of the trachea on reduces on exhalation, as compared with inhalation.
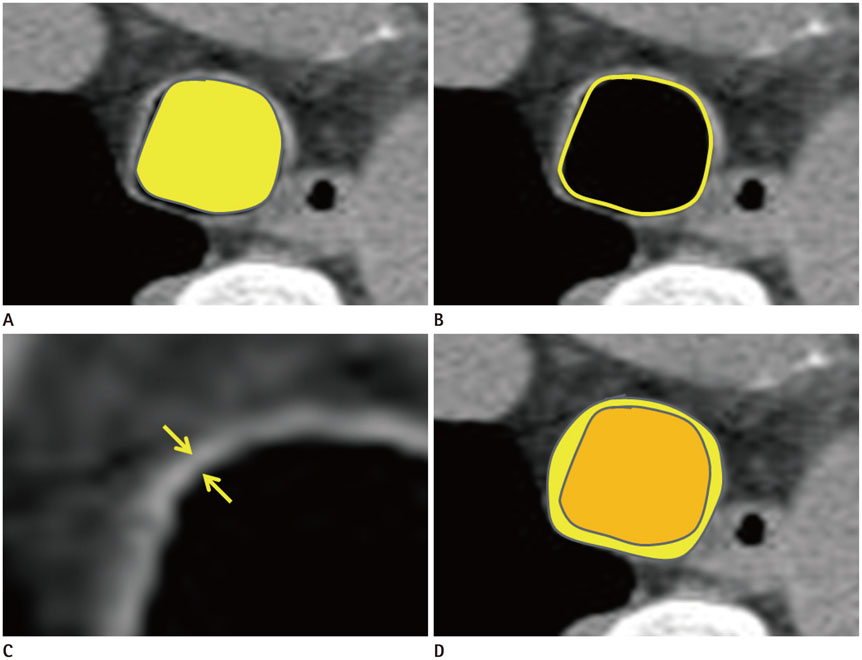
Fig. 2 Quantified four airway parameters of normal 37-year-old woman at inspiration. A. Minimal luminal area: 145.91 mm2. B. Luminal perimeter: 43.36 mm. C. Wall thickness between outer and inner margin (arrow): 2.69 mm. D. Wall to total area ratio: 0.49.
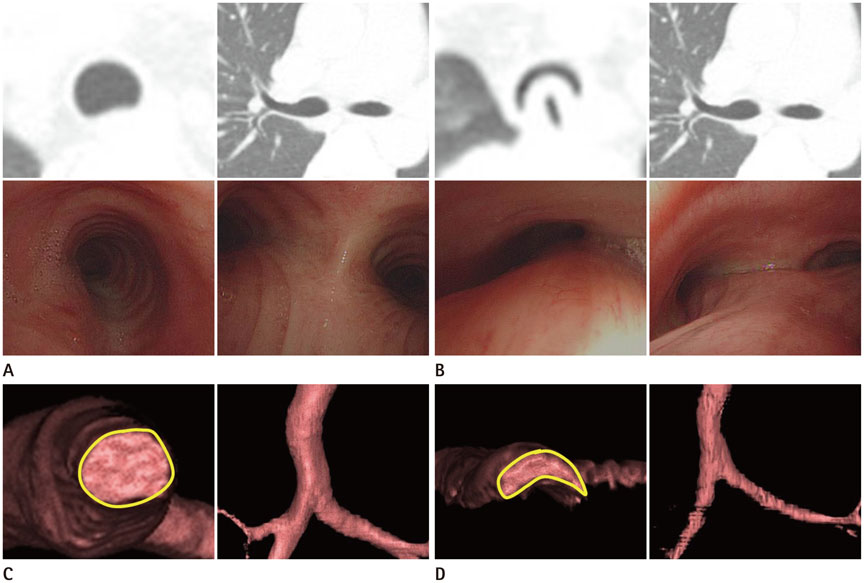
Fig. 3 A 61-year-old woman complained of dyspnea of 2 months duration. She was diagnosed as tracheobronchomalacia by HRCT and bronchoscopy. CT and bronchoscopy images in (A) inspiration and (B) expiration. Luminal area of trachea at expiration is significantly decreased, compared with inspiration. 3D reconstructed VIDA images from HRCT images in (C) inspiration and (D) expiration. All luminal areas, wall thickness and luminal perimeter were calculated automatically by 3D reconstruction. Calculated parameters for inspiration vs. expiration are as follows - minimal luminal area: 108.90 mm2 vs. 21.23 mm2; luminal perimeter: 43.72 mm vs. 23.52 mm; wall thickness: 1.65 mm vs. 1.49 mm; wall to total area ratio: 0.37 vs. 0.54. HRCT = high-resolution computed tomography, 3D = three-dimensional
Reference
-
1. Baxter JD, Dunbar JS. Tracheomalacia. Ann Otol Rhinol Laryngol. 1963; 72:1013–1023.2. Nuutinen J. Acquired tracheobronchomalacia. A clinical study with bronchological correlations. Ann Clin Res. 1977; 9:350–355.3. de Jong PA, Müller NL, Paré PD, Coxson HO. Computed tomographic imaging of the airways: relationship to structure and function. Eur Respir J. 2005; 26:140–152.4. Hackx M, Bankier AA, Gevenois PA. Chronic obstructive pulmonary disease: CT quantification of airways disease. Radiology. 2012; 265:34–48.5. Johnson TH, Mikita JJ, Wilson RJ, Feist JH. Acquired tracheomalacia. Radiology. 1973; 109:576–580.6. Palombini BC, Villanova CA, Araújo E, Gastal OL, Alt DC, Stolz DP, et al. A pathogenic triad in chronic cough: asthma, postnasal drip syndrome, and gastroesophageal reflux disease. Chest. 1999; 116:279–284.7. Jokinen K, Palva T, Sutinen S, Nuutinen J. Acquired tracheobronchomalacia. Ann Clin Res. 1977; 9:52–57.8. Topalovic M, Exadaktylos V, Peeters A, Coolen J, Dewever W, Hemeryck M, et al. Computer quantification of airway collapse on forced expiration to predict the presence of emphysema. Respir Res. 2013; 14:131.9. Schmithorst VJ, Altes TA, Young LR, Franz DN, Bissler JJ, McCormack FX, et al. Automated algorithm for quantifying the extent of cystic change on volumetric chest CT: initial results in lymphangioleiomyomatosis. AJR Am J Roentgenol. 2009; 192:1037–1044.10. Park KJ. Clinical use of chest CT in chronic obstructive pulmonary diseases. Korean J Med. 2009; 77:407–414.11. Jang EH, Sun JS, Kang DK, Park KJ, Park KJ. Emphysema quantification using low dose chest CT: changes in follow-up examinations of asymptomatic smokers. J Korean Soc Radiol. 2012; 66:35–42.12. Nam B, Hwang JH, Lee YM, Park JS, Jou SS, Kim Y. Quantitative CT assessment in chronic obstructive pulmonary disease patients: comparison of the patients with and without consistent clinical symptoms and pulmonary function results. J Korean Soc Radiol. 2015; 73:147–157.13. Gilkeson RC, Ciancibello LM, Hejal RB, Montenegro HD, Lange P. Tracheobronchomalacia: dynamic airway evaluation with multidetector CT. AJR Am J Roentgenol. 2001; 176:205–210.14. Boiselle PM, O'Donnell CR, Bankier AA, Ernst A, Millet ME, Potemkin A, et al. Tracheal collapsibility in healthy volunteers during forced expiration: assessment with multidetector CT. Radiology. 2009; 252:255–262.15. Litmanovich D, O'Donnell CR, Bankier AA, Ernst A, Millett ME, Loring SH, et al. Bronchial collapsibility at forced expiration in healthy volunteers: assessment with multidetector CT. Radiology. 2010; 257:560–567.16. Zhang J, Hasegawa I, Hatabu H, Feller-Kopman D, Boiselle PM. Frequency and severity of air trapping at dynamic expiratory CT in patients with tracheobronchomalacia. AJR Am J Roentgenol. 2004; 182:81–85.17. Loring SH, O'donnell CR, Feller-Kopman DJ, Ernst A. Central airway mechanics and flow limitation in acquired tracheobronchomalacia. Chest. 2007; 131:1118–1124.18. Wailoo M, Emery JL. The trachea in children with respiratory diseases including children presenting as cot deaths. Arch Dis Child. 1980; 55:199–203.19. Wailoo M, Emery JL. Structure of the membranous trachea in children. Acta Anat (Basel). 1980; 106:254–261.20. Kiener M, Koblet H, Wyss F. [Pathology of stenosed bronchial collapse with pulmonary emphysema]. Schweiz Med Wochenschr. 1957; 87:660–663.21. Ikeda S, Hanawa T, Konishi T, Adachi M, Sawai S, Chiba W, et al. [Diagnosis, incidence, clinicopathology and surgical treatment of acquired tracheobronchomalacia]. Nihon Kyobu Shikkan Gakkai Zasshi. 1992; 30:1028–1035.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Four-Dimensional Thoracic CT in Free-Breathing Children
- Successful Management of Tracheobronchomalacia Associated with Empyema Using a Covered Metallic Tracheobronchial Stent: A Case Report
- A Case of Postpneumonectomy Syndrome Treated with Endobronchial Stent
- CT Findings of Central Airway Lesions Causing Airway Stenosis-Visualization and Quantification: A Pictorial Essay
- Multi-Detector Row CT of the Central Airway Disease
