Clin Orthop Surg.
2015 Jun;7(2):217-224. 10.4055/cios.2015.7.2.217.
Risk of Anterior Femoral Notching in Navigated Total Knee Arthroplasty
- Affiliations
-
- 1Department of Orthopedic Surgery, Chonbuk National University Hospital, Research Institute of Clinical Medicine, Chonbuk National University Medical School, Jeonju, Korea. wsi1205@naver.com
- KMID: 2164548
- DOI: http://doi.org/10.4055/cios.2015.7.2.217
Abstract
- BACKGROUND
We retrospectively investigated the prevalence of femoral anterior notching and risk factors after total knee arthroplasty (TKA) using an image-free navigation system.
METHODS
We retrospectively reviewed 148 consecutive TKAs in 130 patients beginning in July 2005. Seventy knees (62 patients) underwent conventional TKA, and 78 knees (68 patients) received navigated TKA. We investigated the prevalence of femoral anterior notching and measured notching depth by conventional and navigated TKA. Additionally, the navigated TKA group was categorized into two subgroups according to whether anterior femoral notching had occurred. The degree of preoperative varus deformity, femoral bowing, and mediolateral suitability of the size of the femoral component were determined by reviewing preoperative and postoperative radiographs. The resection angle on the sagittal plane and the angle of external rotation that was set by the navigation system were checked when resecting the distal femur. Clinical outcomes were compared using range of motion (ROM) and the Hospital for Special Surgery (HSS) and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAX) scores between the two groups.
RESULTS
The prevalence of anterior femoral notching by conventional TKA was 5.7%, and that for navigated TKA was 16.7% (p = 0.037). Mean notching depth by conventional TKA was 2.92 +/- 1.18 mm (range, 1.8 to 4.5 mm) and 3.32 +/- 1.54 mm (range, 1.55 to 6.93 mm) by navigated TKA. Preoperative anterior femoral bowing was observed in 61.5% (p = 0.047) and both anterior and lateral femoral bowing in five cases in notching group during navigated TKA (p = 0.021). Oversized femoral components were inserted in 53.8% of cases (p = 0.035). No differences in clinical outcomes for ROM or the HSS and WOMAX scores were observed between the groups. A periprosthetic fracture, which was considered a notching-related side effect, occurred in one case each in the conventional and navigated TKA groups.
CONCLUSIONS
Surgeons should be aware of the risks associated with anterior femoral notching when using a navigation system for TKA. A modification of the femoral cut should be considered when remarkable femoral bowing is observed.
Keyword
MeSH Terms
Figure
-

Fig. 1 The depth of anterior femoral notching (h) was measured as the distance between the anterior cortex line and anterior cut line of the distal femur.
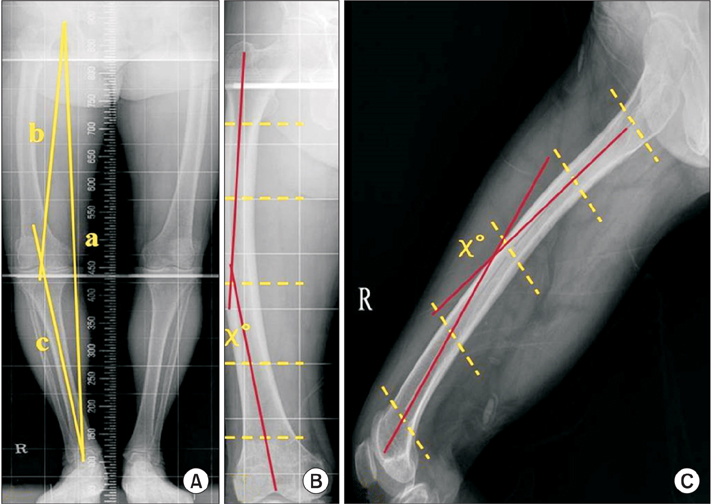
Fig. 2 (A) Standing anteroposterior radiograph of the entire lower limbs. a: mechanical axis of the lower limb, b and c: amount of varus deformity. (B) Lateral bowing of the femur. (C) Anterior bowing of the femoral shaft.
Reference
-
1. Jeffery RS, Morris RW, Denham RA. Coronal alignment after total knee replacement. J Bone Joint Surg Br. 1991; 73(5):709–714.2. Bathis H, Perlick L, Tingart M, Luring C, Zurakowski D, Grifka J. Alignment in total knee arthroplasty: a comparison of computer-assisted surgery with the conventional technique. J Bone Joint Surg Br. 2004; 86(5):682–687.3. Mizu-uchi H, Matsuda S, Miura H, Okazaki K, Akasaki Y, Iwamoto Y. The evaluation of post-operative alignment in total knee replacement using a CT-based navigation system. J Bone Joint Surg Br. 2008; 90(8):1025–1031.4. Sparmann M, Wolke B, Czupalla H, Banzer D, Zink A. Positioning of total knee arthroplasty with and without navigation support: a prospective, randomised study. J Bone Joint Surg Br. 2003; 85(6):830–835.5. Minoda Y, Kobayashi A, Iwaki H, Ohashi H, Takaoka K. TKA sagittal alignment with navigation systems and conventional techniques vary only a few degrees. Clin Orthop Relat Res. 2009; 467(4):1000–1006.6. Minoda Y, Kobayashi A, Iwaki H, et al. The risk of notching the anterior femoral cortex with the use of navigation systems in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2010; 18(6):718–722.7. Lesh ML, Schneider DJ, Deol G, Davis B, Jacobs CR, Pellegrini VD Jr. The consequences of anterior femoral notching in total knee arthroplasty: a biomechanical study. J Bone Joint Surg Am. 2000; 82(8):1096–1101.8. Zalzal P, Backstein D, Gross AE, Papini M. Notching of the anterior femoral cortex during total knee arthroplasty characteristics that increase local stresses. J Arthroplasty. 2006; 21(5):737–743.9. Yau WP, Chiu KY, Tang WM, Ng TP. Coronal bowing of the femur and tibia in Chinese: its incidence and effects on total knee arthroplasty planning. J Orthop Surg (Hong Kong). 2007; 15(1):32–36.10. Aaron RK, Scott R. Supracondylar fracture of the femur after total knee arthroplasty. Clin Orthop Relat Res. 1987; (219):136–139.11. Figgie MP, Goldberg VM, Figgie HE 3rd, Sobel M. The results of treatment of supracondylar fracture above total knee arthroplasty. J Arthroplasty. 1990; 5(3):267–276.12. Ritter MA, Faris PM, Keating EM. Anterior femoral notching and ipsilateral supracondylar femur fracture in total knee arthroplasty. J Arthroplasty. 1988; 3(2):185–187.13. Chauhan SK, Clark GW, Lloyd S, Scott RG, Breidahl W, Sikorski JM. Computer-assisted total knee replacement: a controlled cadaver study using a multi-parameter quantitative CT assessment of alignment (the Perth CT Protocol). J Bone Joint Surg Br. 2004; 86(6):818–823.14. Kim YH, Kim JS, Yoon SH. Alignment and orientation of the components in total knee replacement with and without navigation support: a prospective, randomised study. J Bone Joint Surg Br. 2007; 89(4):471–476.15. Matziolis G, Krocker D, Weiss U, Tohtz S, Perka C. A prospective, randomized study of computer-assisted and conventional total knee arthroplasty: three-dimensional evaluation of implant alignment and rotation. J Bone Joint Surg Am. 2007; 89(2):236–243.16. Egol KA, Chang EY, Cvitkovic J, Kummer FJ, Koval KJ. Mismatch of current intramedullary nails with the anterior bow of the femur. J Orthop Trauma. 2004; 18(7):410–415.17. Nagamine R, Kondo K, Ikemura S, et al. Distal femoral cut perpendicular to the mechanical axis may induce varus instability in flexion in medial osteoarthritic knees with varus deformity in total knee arthroplasty: a pitfall of the navigation system. J Orthop Sci. 2004; 9(6):555–559.18. Stulberg SD. How accurate is current TKR instrumentation? Clin Orthop Relat Res. 2003; (416):177–184.19. Scuderi GR. The stiff total knee arthroplasty: causality and solution. J Arthroplasty. 2005; 20:4 Suppl 2. 23–26.20. Perlick L, Bathis H, Tingart M, Perlick C, Grifka J. Navigation in total-knee arthroplasty: CT-based implantation compared with the conventional technique. Acta Orthop Scand. 2004; 75(4):464–470.21. Hirsh DM, Bhalla S, Roffman M. Supracondylar fracture of the femur following total knee replacement: report of four cases. J Bone Joint Surg Am. 1981; 63(1):162–163.22. Merkel KD, Johnson EW Jr. Supracondylar fracture of the femur after total knee arthroplasty. J Bone Joint Surg Am. 1986; 68(1):29–43.23. Culp RW, Schmidt RG, Hanks G, Mak A, Esterhai JL Jr, Heppenstall RB. Supracondylar fracture of the femur following prosthetic knee arthroplasty. Clin Orthop Relat Res. 1987; (222):212–222.24. Shawen SB, Belmont PJ Jr, Klemme WR, Topoleski LD, Xenos JS, Orchowski JR. Osteoporosis and anterior femoral notching in periprosthetic supracondylar femoral fractures: a biomechanical analysis. J Bone Joint Surg Am. 2003; 85(1):115–121.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Risk Factors of Periprosthetic Fracture after Total Knee Arthroplasty
- Periprosthetic Fractures Following Total Knee Arthroplasty
- Fracture of the Femoral Component after Total Knee Arthroplasty Using Anterior-Posterior Glide Mobile-Bearing System
- Repeated Periprosthethic Femoral Fracture in a Below Knee Amputee with Ipsilateral Cementless Total Hip Arthroplasty: A Case Report
- Acute Arterial Occlusion Following Primary Total Knee Arthroplasty
