The Results of All-Inside Meniscus Repair Using the Viper Repair System Simultaneously with Anterior Cruciate Ligament Reconstruction
- Affiliations
-
- 1Department of Orthopedic Surgery, Wonkwang University School of Medicine, Iksan, Korea. cch@wonkwang.ac.kr
- 2Department of Nursing, Chodang University, Muan, Korea.
- 3Department of Orthopedics Surgery, Philippine Orthopedic Center, Manila, Philippines.
- KMID: 2164542
- DOI: http://doi.org/10.4055/cios.2015.7.2.177
Abstract
- BACKGROUND
Meniscus tears are commonly associated with anterior cruciate ligament (ACL) ruptures. It is essential to repair meniscal tears as much as possible to prevent early osteoarthritis and to gain additional stability in the knee joint. We evaluated the results of arthroscopic all-inside repair using the Meniscal Viper Repair System (Arthrex) on meniscus tears simultaneously with ACL reconstruction.
METHODS
Nineteen out of 22 patients who were treated with arthroscopic all-inside repair using the Meniscal Viper Repair System for meniscus tear associated with ACL rupture were evaluated. ACL reconstructions were performed at the same period. The mean follow-up period was 16.5 months (range, 12 to 24 months). The clinical results of the meniscus repair were evaluated by symptoms (such as catching or locking), tenderness, effusion, range of motion limitation, and the McMurray test. Clinical success was defined by negative results in all five categories. The Hospital for Special Surgery (HSS) score was evaluated. Objective results were evaluated with secondary look arthroscopy or magnetic resonance imaging (MRI). The MRI results were categorized as completely repaired, incompletely repaired, and failure by Henning's classification. The results of second-look arthroscopy were evaluated with the criteria of meniscal healing.
RESULTS
The clinical success rate was 95.4% and the HSS scores were 93.9 +/- 5.4 at the final follow-up. According to Henning's classification, 15 out of 18 cases showed complete healing (83.3%) and two cases (11.1%) showed incomplete healing. Seventeen out of 18 cases that underwent second-look arthroscopy showed complete healing (94.4%) according to the criteria of meniscal healing. Only one case showed failure and the failure was due to a re-rupture at the sutured area. Complications of ACL reconstruction or meniscus repair were not present.
CONCLUSIONS
The results demonstrate that arthroscopic all-inside repair using the Meniscal Viper Repair System is an effective treatment method when it is performed simultaneously with ACL reconstruction.
Keyword
MeSH Terms
Figure
-

Fig. 1 The Meniscal Viper Repair System.

Fig. 2 Patient selection process. ACL: anterior cruciate ligament, MRI: magnetic resonance imaging.

Fig. 3 Healing rates by segment according to Henning's criteria: (A) complete healing, (B) partial healing > 50%, and (C) < 50% healing.
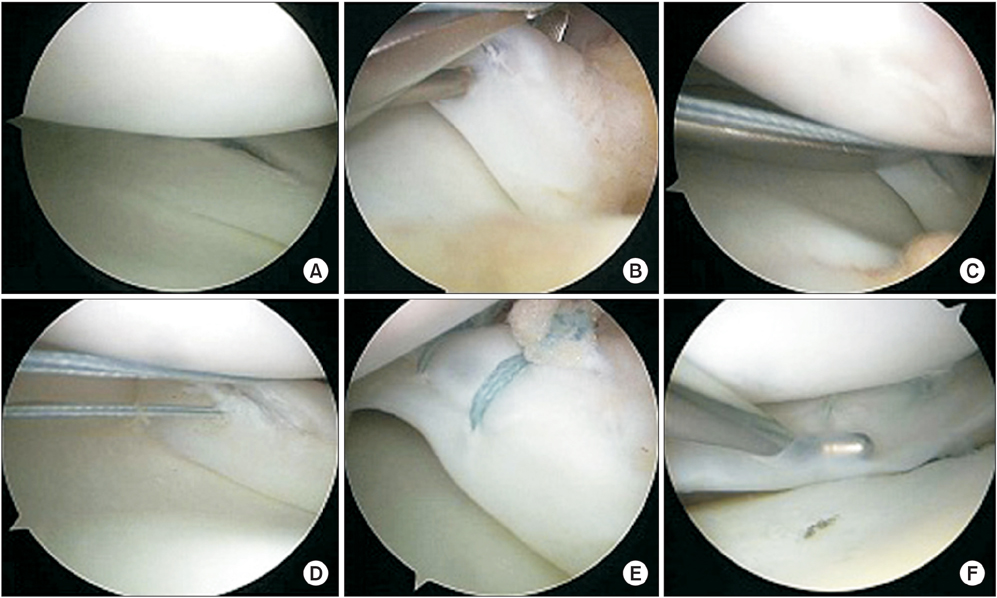
Fig. 4 An 18-year-old woman with a complete rupture of the anterior cruciate ligament and longitudinal tear of the medial meniscus of her left knee. (A) Arthroscopic findings of longitudinal tear of medial meniscus. (B-D) Arthroscopic findings during meniscus repair using the Meniscal Viper Repair System. (E) Arthroscopic finding immediately after suture. (F) Second-look arthroscopic findings after meniscus repair show complete healing.

Fig. 5 A 41-year-old man with complete rupture of the anterior cruciate ligament and longitudinal tear of the lateral meniscus of his right knee. (A) Arthroscopic findings of longitudinal tear of lateral meniscus. (B, C) Arthroscopic findings during meniscus repair using the Meniscal Viper Repair System. (D) Arthroscopic findings immediately after suture. (E) Second-look arthroscopic findings after meniscus repair show complete healing.
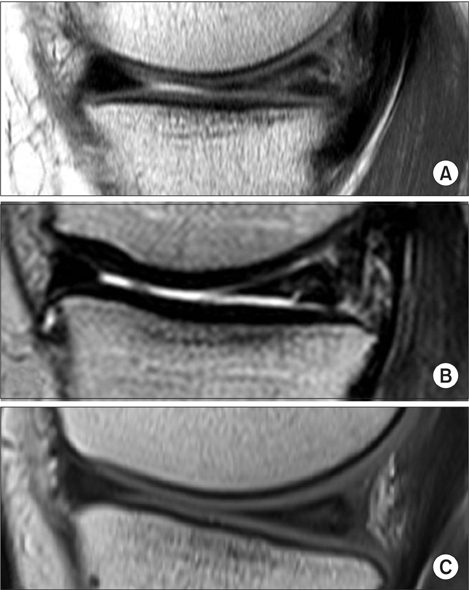
Fig. 6 (A) The preoperative coronal magnetic resonance imaging (MRI) scan revealed a longitudinal tear of the medial meniscus. (B) The follow-up MRI obtained 15 months after the operation shows partial healing at the previous tear of medial meniscus. (C) The MRI at the 24-month follow-up appointment shows almost complete healing at the medial meniscus lesion.
Reference
-
1. DeHaven KE. Diagnosis of acute knee injuries with hemarthrosis. Am J Sports Med. 1980; 8(1):9–14.2. Warren RF, Marshall JL. Injuries of the anterior cruciate and medial collateral ligaments of the knee: a long-term follow-up of 86 cases: part II. Clin Orthop Relat Res. 1978; (136):198–211.3. de Girolamo L, Galliera E, Volpi P, et al. Why menisci show higher healing rate when repaired during ACL reconstruction? Growth factors release can be the explanation. Knee Surg Sports Traumatol Arthrosc. 2015; 23(1):90–96.4. Horibe S, Shino K, Nakata K, Maeda A, Nakamura N, Matsumoto N. Second-look arthroscopy after meniscal repair: review of 132 menisci repaired by an arthroscopic insideout technique. J Bone Joint Surg Br. 1995; 77(2):245–249.5. Kocabey Y, Tetik O, Isbell WM, Atay OA, Johnson DL. The value of clinical examination versus magnetic resonance imaging in the diagnosis of meniscal tears and anterior cruciate ligament rupture. Arthroscopy. 2004; 20(7):696–700.6. Murrell GA, Maddali S, Horovitz L, Oakley SP, Warren RF. The effects of time course after anterior cruciate ligament injury in correlation with meniscal and cartilage loss. Am J Sports Med. 2001; 29(1):9–14.7. Shelbourne KD, Gray T. Results of anterior cruciate ligament reconstruction based on meniscus and articular cartilage status at the time of surgery: five- to fifteen-year evaluations. Am J Sports Med. 2000; 28(4):446–452.8. Warren RF. Meniscectomy and repair in the anterior cruciate ligament-deficient patient. Clin Orthop Relat Res. 1990; (252):55–63.9. Ahn JH, Wang JH, Yoo JC. Arthroscopic all-inside suture repair of medial meniscus lesion in anterior cruciate ligament: deficient knees: results of second-look arthroscopies in 39 cases. Arthroscopy. 2004; 20(9):936–945.10. Rodeo SA. Arthroscopic meniscal repair with use of the outside-in technique. Instr Course Lect. 2000; 49:195–206.11. Johnson D, Weiss B. Meniscal repair using the inside-out suture technique. Sports Med Arthrosc. 2012; 20(2):68–76.12. Vinyard TR, Wolf BR. Meniscal repair: outside-in repair. Clin Sports Med. 2012; 31(1):33–48.13. Kang HJ, Chun CH, Kim SH, Kim KM. A ganglion cyst generated by non-absorbable meniscal repair suture material. Orthop Traumatol Surg Res. 2012; 98(5):608–612.14. Gunes T, Bostan B, Erdem M, Asci M, Sen C, Kelestemur MH. Biomechanical evaluation of arthroscopic all-inside meniscus repairs. Knee Surg Sports Traumatol Arthrosc. 2009; 17(11):1347–1353.15. Pujol N, Tardy N, Boisrenoult P, Beaufils P. Long-term outcomes of all-inside meniscal repair. Knee Surg Sports Traumatol Arthrosc. 2015; 23(1):219–224.16. Hagino T, Ochiai S, Watanabe Y, et al. Clinical results of arthroscopic all-inside lateral meniscal repair using the Meniscal Viper Repair System. Eur J Orthop Surg Traumatol. 2014; 24(1):99–104.17. Kurzweil PR, Tifford CD, Ignacio EM. Unsatisfactory clinical results of meniscal repair using the meniscus arrow. Arthroscopy. 2005; 21(8):905.18. Starke C, Kopf S, Petersen W, Becker R. Meniscal repair. Arthroscopy. 2009; 25(9):1033–1044.19. Chang HC, Caborn DN, Nyland J, Burden R. Effect of lesion location on fixation strength of the meniscal viper repair system: an in vitro study using porcine menisci. Arthroscopy. 2006; 22(4):394–399.20. Henning CE, Clark JR, Lynch MA, Stallbaumer R, Yearout KM, Vequist SW. Arthroscopic meniscus repair with a posterior incision. Instr Course Lect. 1988; 37:209–221.21. Scott GA, Jolly BL, Henning CE. Combined posterior incision and arthroscopic intra-articular repair of the meniscus: an examination of factors affecting healing. J Bone Joint Surg Am. 1986; 68(6):847–861.22. Shelbourne KD, Nitz PA. The O'Donoghue triad revisited: combined knee injuries involving anterior cruciate and medial collateral ligament tears. Am J Sports Med. 1991; 19(5):474–477.23. Gill SS, Diduch DR. Outcomes after meniscal repair using the meniscus arrow in knees undergoing concurrent anterior cruciate ligament reconstruction. Arthroscopy. 2002; 18(6):569–577.24. Cerabona F, Sherman MF, Bonamo JR, Sklar J. Patterns of meniscal injury with acute anterior cruciate ligament tears. Am J Sports Med. 1988; 16(6):603–609.25. Sherman MF, Lieber L, Bonamo JR, Podesta L, Reiter I. The long-term followup of primary anterior cruciate ligament repair: defining a rationale for augmentation. Am J Sports Med. 1991; 19(3):243–255.26. Noyes FR, Barber-Westin SD. Treatment of meniscus tears during anterior cruciate ligament reconstruction. Arthroscopy. 2012; 28(1):123–130.27. Shelbourne KD, Carr DR. Meniscal repair compared with meniscectomy for bucket-handle medial meniscal tears in anterior cruciate ligament-reconstructed knees. Am J Sports Med. 2003; 31(5):718–723.28. Bellabarba C, Bush-Joseph CA, Bach BR Jr. Patterns of meniscal injury in the anterior cruciate-deficient knee: a review of the literature. Am J Orthop (Belle Mead NJ). 1997; 26(1):18–23.29. Belzer JP, Cannon WD Jr. Meniscus tears: treatment in the stable and unstable knee. J Am Acad Orthop Surg. 1993; 1(1):41–47.30. Lee DW, Jang HW, Lee SR, Park JH, Ha JK, Kim JG. Clinical, radiological, and morphological evaluations of posterior horn tears of the lateral meniscus left in situ during anterior cruciate ligament reconstruction. Am J Sports Med. 2014; 42(2):327–335.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Patellar Tendon Rupture associated with Rupture of Anterior Cruciate Ligament, Both Collateral Ligoments, and Lateral Meniscus: A Case Report
- Reconstruction of the Posterior Cruciate Ligament Using the Medial Meniscus
- Open anterior cruciate ligament reconstruction using inside-out femoral drilling
- Anomalous Insertion of the Anterior Medial Meniscus
- The Primary Repair of Acute Anterior Cruciate Ligament Injury
