Twenty-Year Experience of a Double-Bundle Anterior Cruciate Ligament Reconstruction
- Affiliations
-
- 1Department of Joint Surgery and Sports Medicine, Graduate School of Medicine, Tokyo Medical and Dental University, Tokyo, Japan. muneta.orj@tmd.ac.jp
- KMID: 2164537
- DOI: http://doi.org/10.4055/cios.2015.7.2.143
Abstract
- Double-bundle (DB) anterior cruciate ligament (ACL) reconstruction using a four-strand semitendinosus tendon was started in our department in July 1994. The motivation for starting the procedure was that the EndoButton with an inside-out procedure instrument became available in Japan. A review article of our DB ACL reconstruction procedure was summarized for the twentieth anniversary of the surgical procedure. Initial tension setting of the two grafts was changed in the first 8 years to achieve better stability during DB ACL reconstruction. A randomized clinical trial (RCT) was started in July 2002 to clarify superiority of the DB procedure to single-bundle (SB) reconstruction under the concept of anatomic reconstruction. Several anatomic studies were performed to describe normal ACL anatomy, which is essential for realizing anatomic reconstruction. A remnant-preserving technique would be an additional option for our DB procedure to improve reconstruction outcomes. Thus, a new remnant-preserving DB procedure was started in 2012. The reproducibility of the new procedure was investigated using three-dimensional computed tomography images. More complex procedures were performed using a transtibial technique and EndoButtons. Initial tension balancing between the two grafts was important for a better outcome. Superiority of knee stability after the DB compared to that after the SB procedure was clarified by the RCT. However, no patient consensus has been reached on any subjective advantage to the DB procedure. Studies of normal ACL anatomy have left questions unresolved regarding where the two tunnels should be created for direct and indirect insertions based on normal anatomy. A new remnant-preserving DB ACL procedure has been practiced. The procedure was more reproducible with respect to creating the femoral tunnel. DB ACL reconstruction using a semitendinosus tendon is an attractive option when pursuing a better outcome for patients.
Figure
-
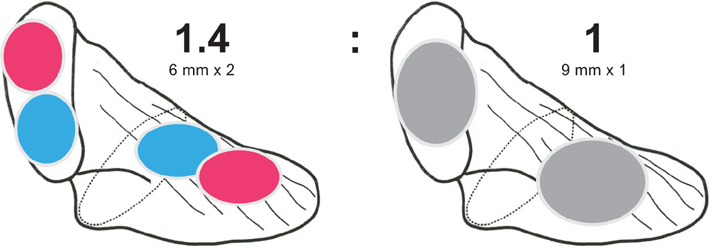
Fig. 1 A greater tendon-bone junction area is achieved with the double-bundle (DB) technique. DB reconstruction features: (1) greater tendon-bone junction area facilitating better stabilization of the graft, (2) greater tendon-bone junction area facilitating graft healing, (3) less anterior notch plasty, and (4) the possibility to realize ideal initial graft settings.
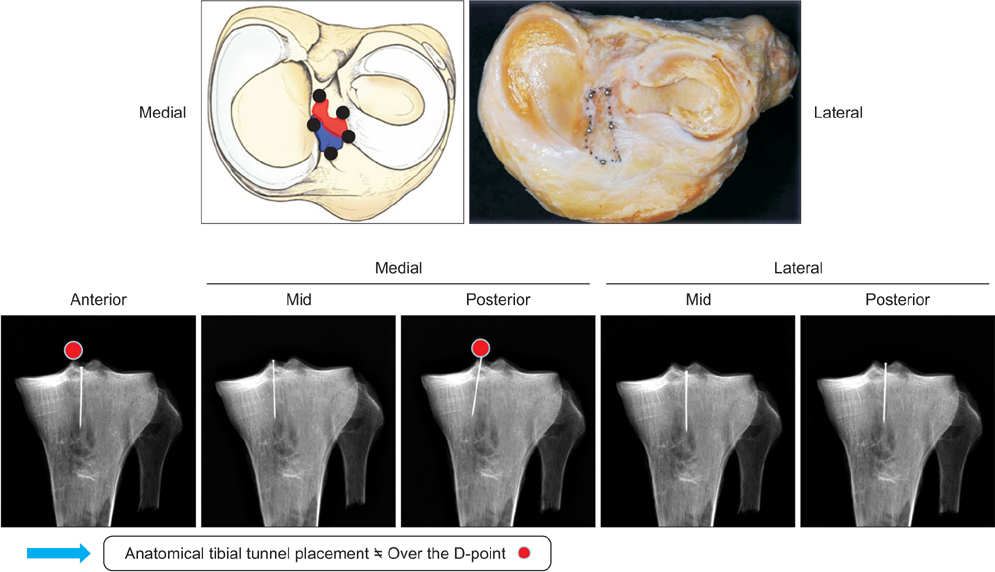
Fig. 2 Tibial drill hole placement: anatomic landmarks and radiographic findings. Guidewires should not be placed over the D-point laterally.
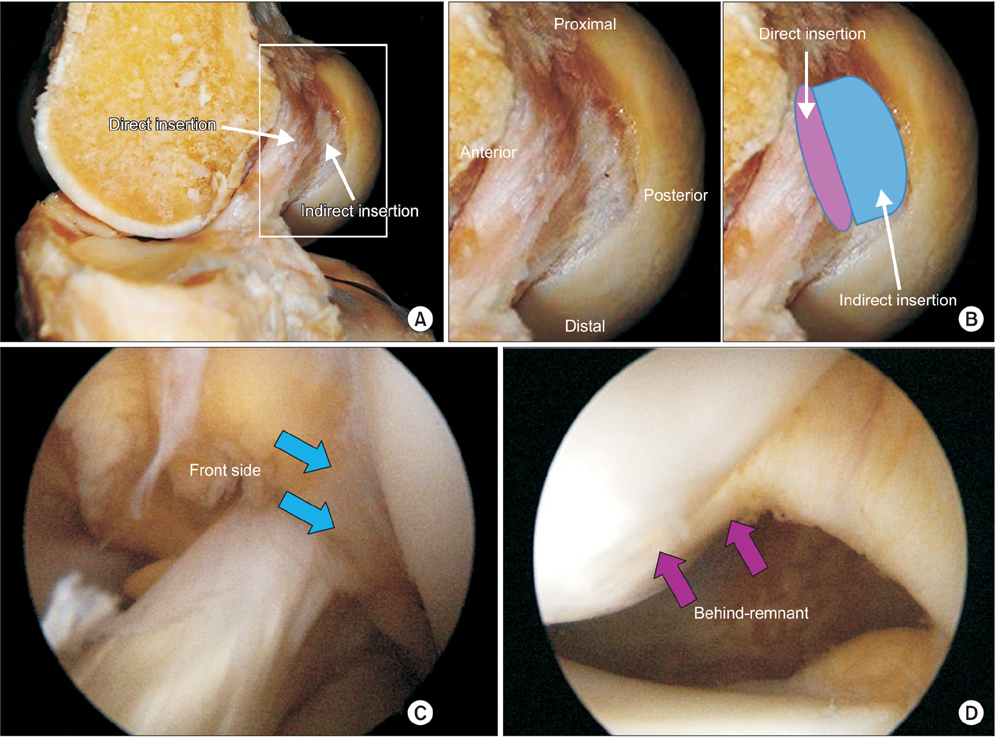
Fig. 3 Normal anterior cruciate ligament (ACL) anatomy. (A) Direct insertion is bundle-like and exists on the lateral wall of the intercondylar notch. (B) Indirect insertion is membranous in cadaveric knees and its ligamentous function has not been well evaluated. (C) Arthroscopic observation of normal femoral ACL femoral attachment. A normal ACL consists of direct and indirect insertions. (D) The insertions cannot be separated with continuous extension from the articular surface.

Fig. 4 (A, B) The front side of an injured anterior cruciate ligament (ACL). Particularly, the anteromedial portion is rather preserved as a roof of the femoral attachment in two cases. Blue arrows indicate anterior border of the ACL. (C, D) Two cases of findings behind the remnant of an injured ACL. The posterior part of the ACL remnant is an indirect insertion, and it is ruptured and scarred with some inflammation in two cases. Pink arrows indicate scarred indirect insertion with synovial tissue.
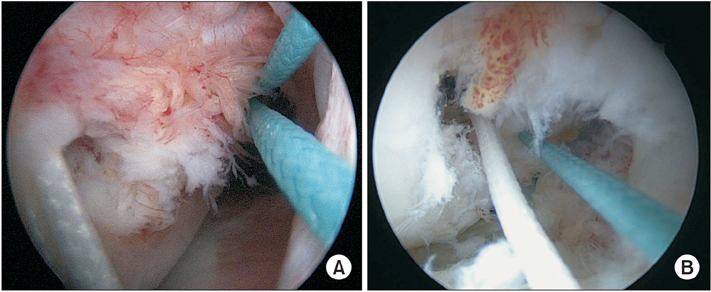
Fig. 5 (A, B) Two cases of anteromedial and posterolateral femoral tunnels created behind the remnant.
Reference
-
1. Muneta T, Sekiya I, Yagishita K, Ogiuchi T, Yamamoto H, Shinomiya K. Two-bundle reconstruction of the anterior cruciate ligament using semitendinosus tendon with endobuttons: operative technique and preliminary results. Arthroscopy. 1999; 15(6):618–624.2. Muneta T, Sekiya I, Ogiuchi T, Yagishita K, Yamamoto H, Shinomiya K. Effects of aggressive early rehabilitation on the outcome of anterior cruciate ligament reconstruction with multi-strand semitendinosus tendon. Int Orthop. 1998; 22(6):352–356.3. Yamamoto H, Ishibashi T, Muneta T, Furuya K, Mizuta T. Effusions after anterior cruciate ligament reconstruction using the ligament augmentation device. Arthroscopy. 1992; 8(3):305–310.4. Muneta T, Sekiya I, Ogiuchi T, Yagishita K, Yamamoto H, Shinomiya K. Objective factors affecting overall subjective evaluation of recovery after anterior cruciate ligament reconstruction. Scand J Med Sci Sports. 1998; 8(5 Pt 1):283–289.5. Hefzy MS, Grood ES, Noyes FR. Factors affecting the region of most isometric femoral attachments. Part II: the anterior cruciate ligament. Am J Sports Med. 1989; 17(2):208–216.6. Yamazaki J, Muneta T, Koga H, et al. Radiographic description of femoral tunnel placement expressed as intercondylar clock time in double-bundle anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2011; 19(3):418–423.7. Howell SM, Clark JA, Farley TE. A rationale for predicting anterior cruciate graft impingement by the intercondylar roof: a magnetic resonance imaging study. Am J Sports Med. 1991; 19(3):276–282.8. Muneta T, Koga H, Morito T, Yagishita K, Sekiya I. A retrospective study of the midterm outcome of two-bundle anterior cruciate ligament reconstruction using quadrupled semitendinosus tendon in comparison with one-bundle reconstruction. Arthroscopy. 2006; 22(3):252–258.9. Muneta T, Koga H, Ju YJ, Yagishita K, Sekiya I. Effects of different initial bundle tensioning strategies on the outcome of double-bundle ACL reconstruction: a cohort study. Sports Med Arthrosc Rehabil Ther Technol. 2011; 3(1):15.10. Koga H, Muneta T, Yagishita K, et al. Effect of posterolateral bundle graft fixation angles on clinical outcomes in double-bundle anterior cruciate ligament reconstruction: a randomized controlled trial. Am J Sports Med. 2015; Feb. 2. [Epub]. http://dx.doi.org/10.1177/0363546514567069.11. Muneta T, Koga H, Mochizuki T, et al. A prospective randomized study of 4-strand semitendinosus tendon anterior cruciate ligament reconstruction comparing single-bundle and double-bundle techniques. Arthroscopy. 2007; 23(6):618–628.12. Tiamklang T, Sumanont S, Foocharoen T, Laopaiboon M. Double-bundle versus single-bundle reconstruction for anterior cruciate ligament rupture in adults. Cochrane Database Syst Rev. 2012; 11:CD008413.13. Xu M, Gao S, Zeng C, et al. Outcomes of anterior cruciate ligament reconstruction using single-bundle versus double-bundle technique: meta-analysis of 19 randomized controlled trials. Arthroscopy. 2013; 29(2):357–365.14. Koga H, Muneta T, Yagishita K, et al. Mid- to long-term results of single-bundle versus double-bundle anterior cruciate ligament reconstruction: randomized controlled trial. Arthroscopy. 2015; 31(1):69–76.15. Araki D, Kuroda R, Kubo S, et al. A prospective randomised study of anatomical single-bundle versus double-bundle anterior cruciate ligament reconstruction: quantitative evaluation using an electromagnetic measurement system. Int Orthop. 2011; 35(3):439–446.16. Hemmerich A, van der Merwe W, Batterham M, Vaughan CL. Knee rotational laxity in a randomized comparison of single- versus double-bundle anterior cruciate ligament reconstruction. Am J Sports Med. 2011; 39(1):48–56.17. Mochizuki T, Muneta T, Nagase T, Shirasawa S, Akita KI, Sekiya I. Cadaveric knee observation study for describing anatomic femoral tunnel placement for two-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2006; 22(4):356–361.18. Hara K, Mochizuki T, Sekiya I, Yamaguchi K, Akita K, Muneta T. Anatomy of normal human anterior cruciate ligament attachments evaluated by divided small bundles. Am J Sports Med. 2009; 37(12):2386–2391.19. Iwahashi T, Shino K, Nakata K, et al. Direct anterior cruciate ligament insertion to the femur assessed by histology and 3-dimensional volume-rendered computed tomography. Arthroscopy. 2010; 26:9 Suppl. S13–S20.20. Sasaki N, Ishibashi Y, Tsuda E, et al. The femoral insertion of the anterior cruciate ligament: discrepancy between macroscopic and histological observations. Arthroscopy. 2012; 28(8):1135–1146.21. Mochizuki T, Fujishiro H, Nimura A, et al. Anatomic and histologic analysis of the mid-substance and fan-like extension fibres of the anterior cruciate ligament during knee motion, with special reference to the femoral attachment. Knee Surg Sports Traumatol Arthrosc. 2014; 22(2):336–344.22. Muneta T, Koga H, Ju YJ, Horie M, Nakamura T, Sekiya I. Remnant volume of anterior cruciate ligament correlates preoperative patients' status and postoperative outcome. Knee Surg Sports Traumatol Arthrosc. 2013; 21(4):906–913.23. Bernard M, Hertel P, Hornung H, Cierpinski T. Femoral insertion of the ACL: radiographic quadrant method. Am J Knee Surg. 1997; 10(1):14–21.24. Muneta T, Koga H, Nakamura T, et al. A new behind-remnant approach for remnant-preserving double-bundle anterior cruciate ligament reconstruction compared with a standard approach. Knee Surg Sports Traumatol Arthrosc. 2014; Sep. 11. [Epub]. http://dx.doi.org/10.1007/s00167-014-3300-2.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Trends in Anterior Cruciate Ligament Reconstruction
- Double-Bundle Anterior Cruciate Ligament Reconstruction
- Single Bundle Anterior Cruciate Ligament Reconstruction
- What Has Been Learned in Anterior Cruciate Ligament Reconstruction during the Past 20 Years?
- Clinical and Radiologic Results of Transtibial Single Bundle Reconstruction and Double Bundle Reconstruction of the Posterior Cruciate Ligament Using the Allo-achilles Tendon
