Pediatr Infect Vaccine.
2016 Apr;23(1):40-45. 10.14776/piv.2016.23.1.40.
Etiology of Acute Pharyngotonsillitis in Children: The Presence of Viruses and Bacteria
- Affiliations
-
- 1Department of Pediatrics, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 2Department of Pediatrics, Fatima Hospital, Changwon, Korea. pedma@naver.com
- 3Division of Bacterial Respiratory Infections, Center for Infectious Diseases, Korea National Institute of Health, Seoul, Korea.
- KMID: 2163222
- DOI: http://doi.org/10.14776/piv.2016.23.1.40
Abstract
- PURPOSE
The purpose of this study was to investigate the etiology of acute pharygotonsillitis in pediatric patients.
METHODS
Pharyngeal swabs from patients with acute pharyngotonsillitis were evaluated for viruses and bacterial organisms from March 2010 through March 2011.
RESULTS
Of 615 patients, potentially pathogenic bacteria were isolated in 40 (6.5%), viruses were isolated in 310 (50.4%), and no pathogens were isolated in 267 patients (43.4%). Both viral and bacterial pathogens were found in 2 (0.3%). Of 40 patients with bacterial pathogens, group A streptococci were found in 31 (77.5%). Among 310 patients with virus infection, adenovirus was the most frequently recovered (203 patients; 65.5%), followed by rhinovirus (65 patients; 21.0%), enterovirus (43 patients; 13.9%) and coronavirus (18 patients; 5.8%). There were 25 patients who had been coinfected with 2 viruses. In viral pharyngotonsillitis, cough, rhinorrhea, conjunctivitis and diarrhea were prominent. On the other hand, pharyngeal injection and pharyngeal petechiae were prominent in bacterial pharyngotonsillitis.
CONCLUSIONS
Virus infection was a big part of acute pharyngotonsillitis and there were differences in clinical manifestations among viral and bacterial infections. Therefore, we need to distinguish between virus infection and bacterial infection using clinical signs for preventing the abuse of antibiotics.
Keyword
MeSH Terms
Figure
-
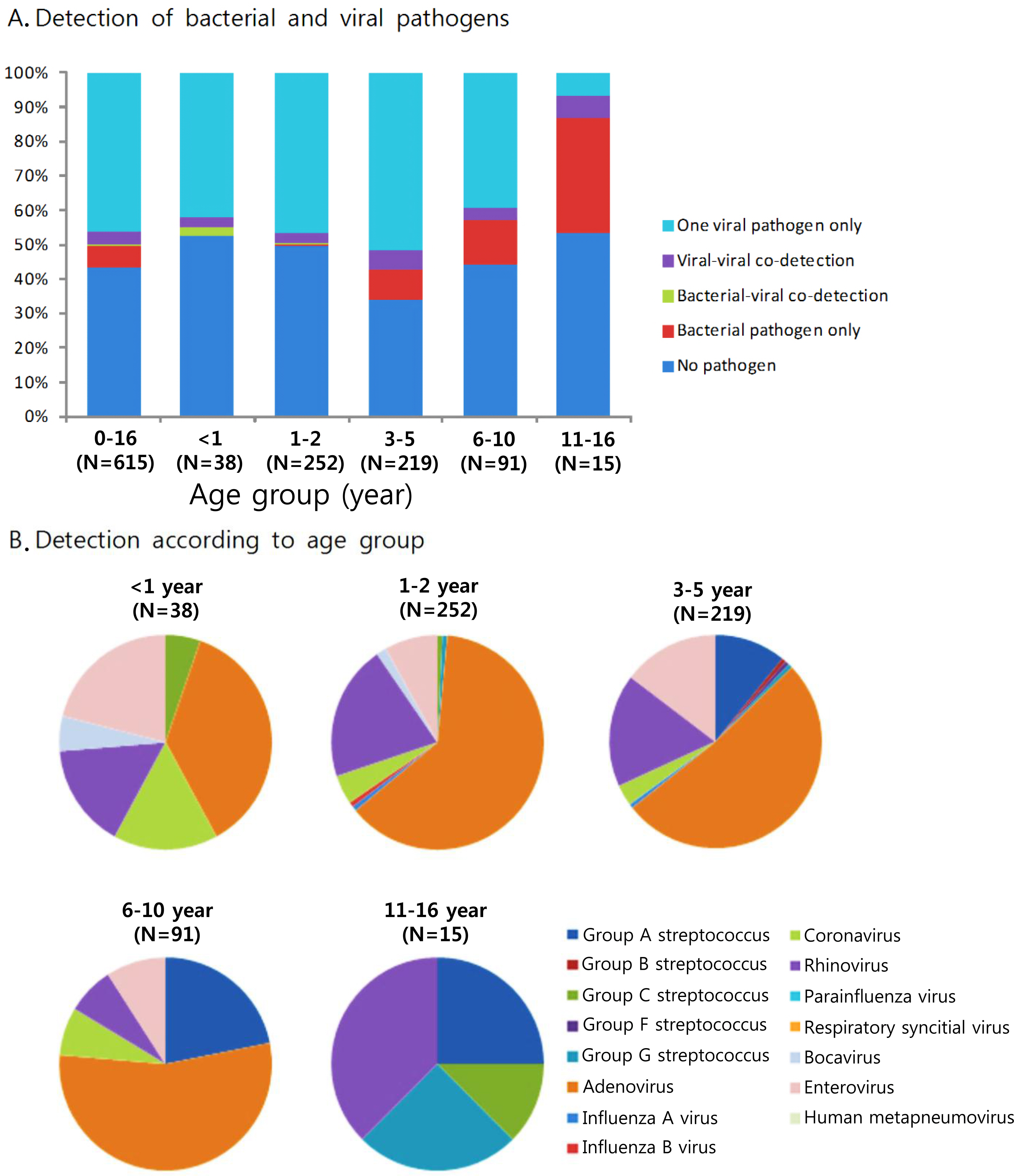
Fig. 1. Microbial findings with aucte pharyngotonsillitis according to patient's age groups, March 2010 to March 2011 (N=615).
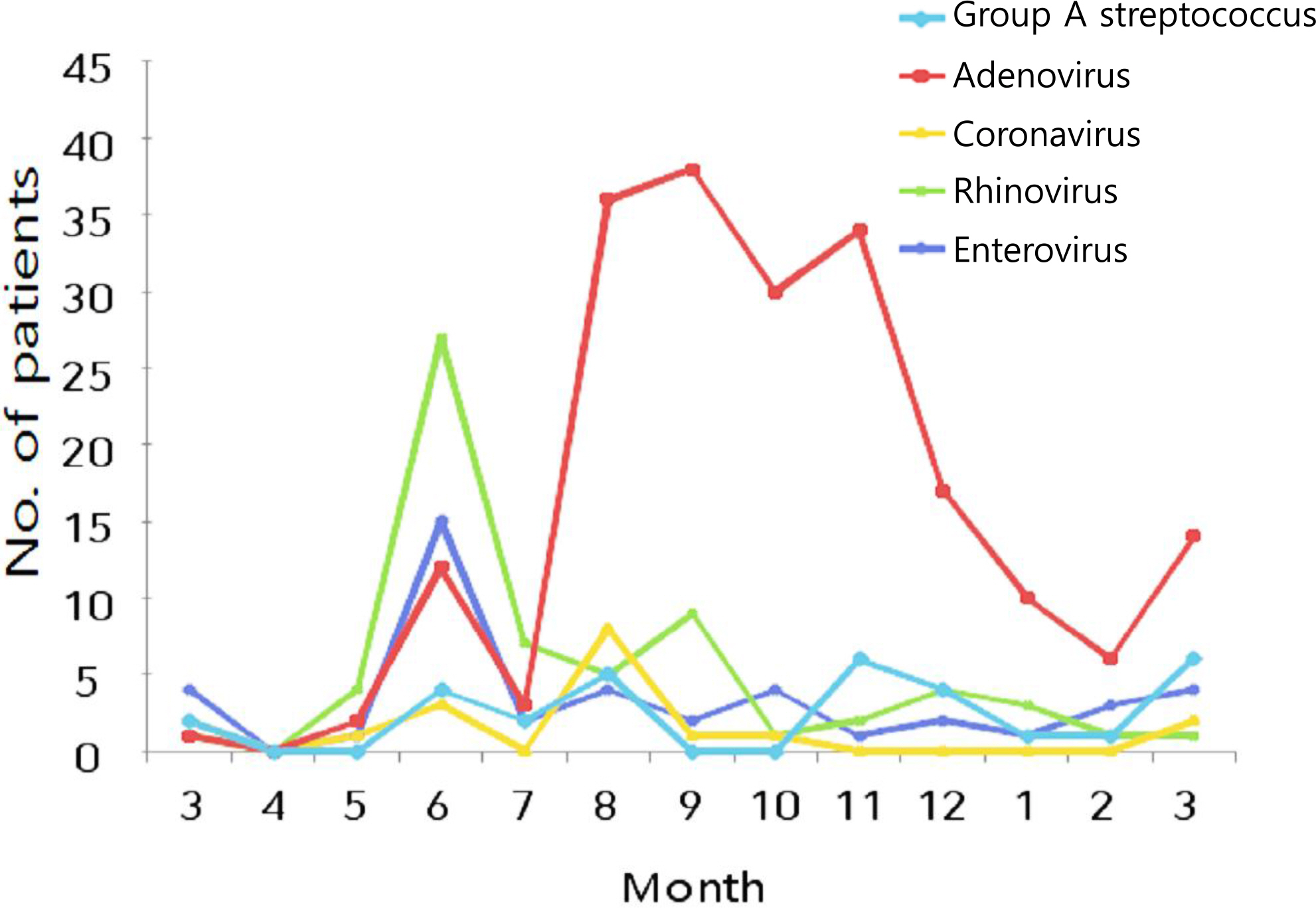
Fig. 2. Monthly distribution of Group A streptococcus, adenovirus, coronavirus, rhinovirus and enterovirus in pediatric patients with acute pharyngotonsillitis, March 2010-March 2011.
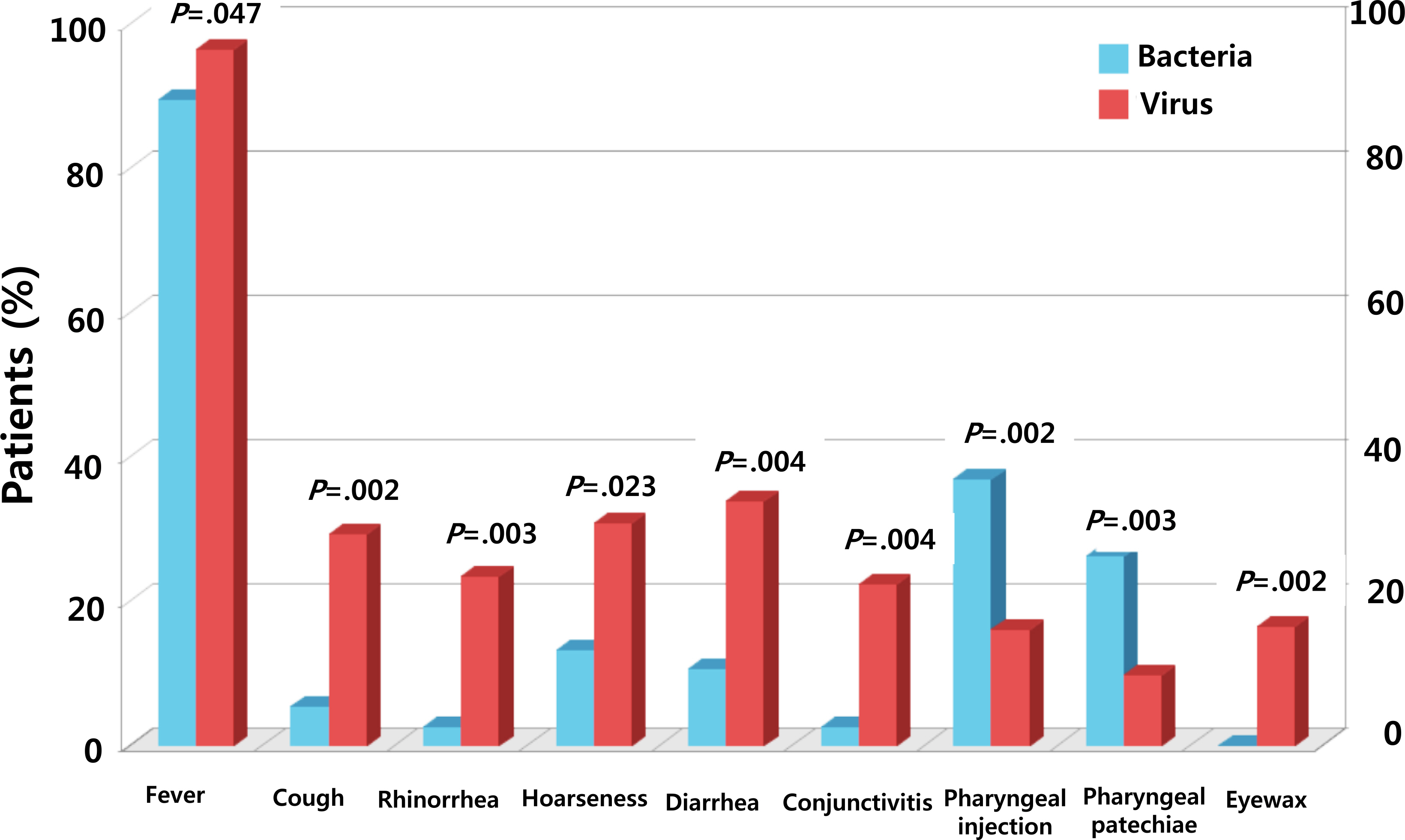
Fig. 3. Symptoms and physical findings in pediatric patients with acute pharyngotonsillitis, according to microbial agents (bacteria or virus).
Reference
-
1. Bisno AL. Acute pharyngitis. N Engl I Med. 2001; 344:205–1. 1.
Article2. Woodwell D. Office visits to pediatric specialists, 1989, Advance data from Vital and health statistics; no 208. Hyattsville. Maryland: National Center for Health Statistics;1992.3. National Health Insurance Service. Acute pharyngotonsillitis. Seoul: National Health Insurance Service, February 22;2015.4. Bae SM. Respiratory bacteria and viruses in the etiology of acute pharyngitis in Korea. PHWR. 2012; 5:58–62.5. Gwaltney JM Jr, Bisno AL. Pharyngitis. Mandel] GL, Bennett IE, Dolin R, editors. editors.Mandell, Douglas and Bennett's principles and practice of infectious diseases. 5th ed.Philadelphia: Churchill Livingstone;2006. p. 656–62.6. Tsou TP, Tan BF, Chang HY, Chen WC, Huang YP, Lai CY, et al. Community outbreak of adenovirus, Taiwan, 2011. Emerg Infect Dis. 2012; 18:1825–32.
Article7. Hsieh TH, Chen PY, Huang FL, Wang ID, Wang LC, Lin HK, et al. Are empiric antibiotics for acute exudative tonsillitis needed in children? J Microbiol Immunol Infect. 2011; 44:328–322.
Article8. Putto A. Febrile exudative tonsillitis: Viral or streptococcal? Pediatrics. 1987; 80:6–12.
Article9. Appenzeller C, Ammann RA, Duppenthaler A, Gorgievski-Hrisoho M, Aebi C. Serum C—reactive protein in children with adenovirus infection. Swiss Med Wkly. 2002; 132:345–50.10. Gerber MA. Diagnosis and treatment of pharyngitis in children. Pediatr Clin North Am. 2005; 52:729–47.
Article11. Dajani A, Taubert K, Ferrieri P, Peter G, Shulman S. Treatment of acute streptococcal pharyngitis and prevention of rheumatic fever: a statement for health professionals. Pediatrics. 1995; 96:758–64.
Article12. Tanz RR. Acute pharyngitis. Kliegman RM, Stanton BMD, St. Geme I, Schor NF, editors. editors.Nelson textbook of pediatrics. 20th ed. Philadelphia: Elsevier, Inc.;2016. p. 2017–21.13. Brien IH, Base IW. Streptococcal pharyngitis: optimal site for throat culture. I Pediatr. 1985; 106:781–3.
Article14. Gerber MA, Shulman ST. Rapid diagnosis of pharyngitis caused by group A streptococci. Clin Microbiol Rev. 2004; 17:571–80.
Article15. Tanz RR, Gerber MA, Kabat W, Rippe I, Seshadri R, Shulman ST. Performance of a rapid antigen-detection test and throat culture in community pediatric offices: implications for management of pharyngitis. Pediatrics. 2009; 123:437–44.
Article16. Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012; 55:1279–82.
Article17. McIsaac W]. White D, Tannenbaum D, Low DE. A clinical score to reduce unnecessary antibiotic use in patients with sore throat. CMAJ. 1998; 158:75–83.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Causes of acute gastroenteritis in Korean children between 2004 and 2019
- Etiology and Clinical Features of Acute Viral Lower Respiratory Tract Infection in Apparently Healthy children
- Community-acquired pneumonia in children: updated perspectives on its etiology, diagnosis, and treatment
- Viral Infections and Associated Factors That Promote Acute Exacerbations of Asthma
- Detection of Respiratory Viruses and Atypical Bacterial Pathogens in Infants with Acute Respiratory Infections Using Multiplex PCR
