Use of Triple Microcatheters for Endovascular Treatment of Wide-Necked Intracranial Aneurysms: A Single Center Experience
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul 03080, Korea. aronnn@empal.com
- 2Department of Neurosurgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul 03080, Korea.
- 3Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul 06351, Korea.
- 4Department of Neurosurgery, Kangwon National University Hospital, Kangwon National University College of Medicine, Chuncheon 24289, Korea.
- KMID: 2160779
- DOI: http://doi.org/10.3348/kjr.2015.16.5.1109
Abstract
OBJECTIVE
The dual microcatheter technique is common practice for coil embolization of a wide-necked aneurysm, due to safety and efficacy. However, technical limitations of some complex configurations may necessitate additional microcatheters to bolster coil stability, compact the coil, or for protection. Described herein is a triple microcatheter technique for endovascular management of wide-necked intracranial aneurysms.
MATERIALS AND METHODS
Data accruing prospectively between January 2006 and October 2014 on simultaneously executed triple microcatheter coil embolization procedures done in 38 saccular aneurysms were reviewed. Clinical and morphological outcomes were assessed, with emphasis on technical aspects of treatment.
RESULTS
The triple microcatheter technique was successfully applied to all 38 saccular aneurysms, involving the posterior communicating artery (n = 13), the middle cerebral artery (n = 10), the basilar tip (n = 7), the anterior cerebral artery (n = 5), and the internal carotid artery (n = 3). Stent protection was added in four patients and balloon remodeling in one. Dual microcatheters (n = 24) were usually deployed to deliver the coil within sacs of aneurysms, with the additional microcatheter used for protection. Otherwise, triple microcatheters were deployed for coil delivery (n = 11) or coils were delivered via a single microcatheter, with dual microcatheters deployed for protection (n = 3). Successful occlusion of aneurysms was achieved in 89.5% of cases, with no procedure-related morbidity or mortality. Stable occlusion was maintained in 72.2% (26/36) of the aneurysms at the final follow-up (mean interval, 30.2 +/- 22.7 months).
CONCLUSION
The outcomes of this limited study suggest that the triple microcatheter technique may be an effective and safe therapeutic option for wide-necked aneurysms, using technical strategies tailored to complex angio-anatomic configurations.
Keyword
MeSH Terms
Figure
-
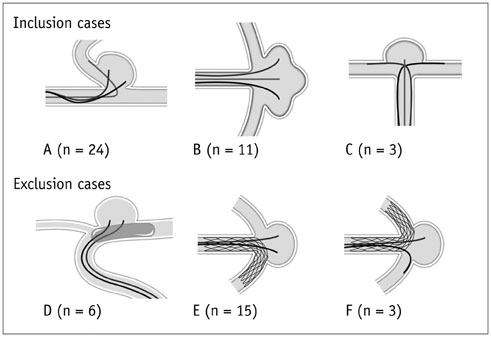
Fig. 1 Schematic depiction of inclusion/exclusion criteria used to study use of simultaneous triple microcatheters. A-C. Eligible patients. A. Dual microcatheters for delivering coil within aneurysmal sac and single microcatheter for protection. B. Triple microcatheter delivery of coil within aneurysm. C. Single microcatheter for delivering coil within aneurysmal sac and dual microcatheters for protection. D-F. Ineligible patients. D. Balloon remodeling and dual microcatheters for delivering coil. E. Stent protection and dual microcatheters for delivering coil (both microcatheters jailed). F. Stent protection and microcatheter protective technique (both microcatheters jailed).
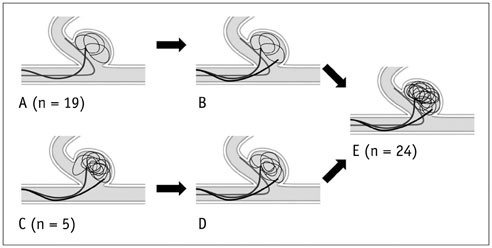
Fig. 2 Schematic illustration (I) of technical strategies using triple microcatheter technique based on angio-anatomical configuration: dual microcatheters for delivering coil within aneurysmal sac and single microcatheter for protection. A. Unstable coil frame (without protrusion) configured via microcatheter protective technique. B. Microcatheter added for delivering coil into aneurysmal sac. C. Coil impingement on branching artery with dual microcatheters. D. Microcatheter added to protect branching artery. E. Proper coil frame configuration by combining dual microcatheter delivery of coil with single microcatheter protection.
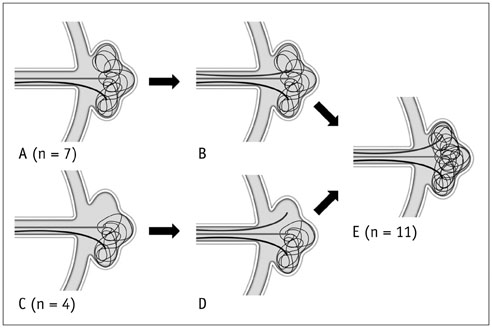
Fig. 3 Schematic illustration (II) of technical strategies using triple microcatheter technique based on angio-anatomical configuration: triple microcatheter delivery of coil within aneurysm. A. Unstable coil frame configured using dual microcatheter technique. B. Microcatheter added to supplement delivery of coil into aneurysmal sac. C. Portion of aneurysm left unfilled by initially delivering coil frame with dual microcatheters (despite proper configuration and no coil protrusion). D. Additional microcatheter placed within void. E. Proper coil frame configuration within aneurysm using triple microcatheter technique.

Fig. 4 Schematic illustration (III) of technical strategies using triple microcatheter technique based on angio-anatomical configuration: single microcatheter for coil delivery within aneurysmal sac and dual microcatheters for protection. A. Coil protruding into unprotected branching artery using microcatheter protective technique. B. Additional microcatheter inserted to protect exposed branch. C. Proper coil frame configured by combining single microcatheter delivery of coil using dual microcatheters for protection.
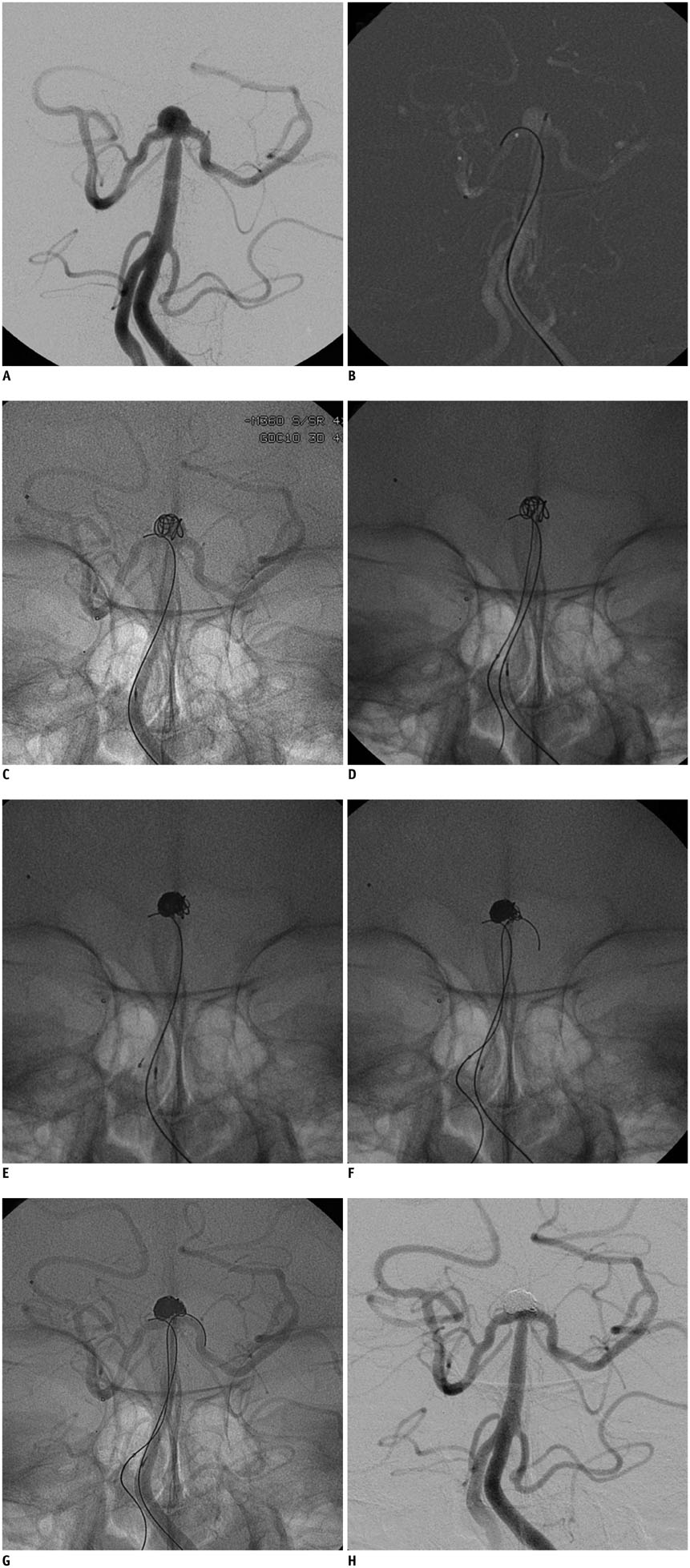
Fig. 5 Illustrative case 1. A. Wide-necked basilar tip aneurysm seen on conventional angiography (note incorporation of both posterior cerebral artery [PCA] orifices by aneurysm). B, C. Coil frame (no protrusion but unstable) configured using microcatheter protective technique (right PCA). D. Microcatheter added to aneurysmal sac through additional guiding catheter in contralateral vertebral artery. E. Intractable coil protrusion (left posterior cerebral artery [PCA]) during delivery of filler coil. F. Microcatheter repositioned from aneurysmal sac to left PCA for protection. G. Coil added via single microcatheter under dual microcatheter protection. H. Complete occlusion of aneurysm.

Fig. 6 Illustrative case 2. A. Middle cerebral artery (MCA) bifurcation aneurysm on conventional angiography (note incorporation of inferior division of MCA by wide-necked shallow aneurysm). B. Dual microcatheters positioned in inferior aneurysmal sac. C, D. Proper coil frame (without protrusion) configured with dual microcatheters, leaving void in superior aneurysmal sac. E, F. Microcatheter added to superior aneurysmal sac, creating supplemental and initial coil frame mix. G. After withdrawing one microcatheter (inferior side), coil was added via dual microcatheters to successfully occlude aneurysm. H. Stably occluded aneurysm 6-month follow-up angiography.
Reference
-
1. Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimpton J, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet. 2002; 360:1267–1274.2. Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003; 362:103–110.3. Shapiro M, Babb J, Becske T, Nelson PK. Safety and efficacy of adjunctive balloon remodeling during endovascular treatment of intracranial aneurysms: a literature review. AJNR Am J Neuroradiol. 2008; 29:1777–1781.4. Pierot L, Cognard C, Spelle L, Moret J. Safety and efficacy of balloon remodeling technique during endovascular treatment of intracranial aneurysms: critical review of the literature. AJNR Am J Neuroradiol. 2012; 33:12–15.5. Biondi A, Janardhan V, Katz JM, Salvaggio K, Riina HA, Gobin YP. Neuroform stent-assisted coil embolization of wide-neck intracranial aneurysms: strategies in stent deployment and midterm follow-up. Neurosurgery. 2007; 61:460–468. discussion 468-4696. Lee SJ, Cho YD, Kang HS, Kim JE, Han MH. Coil embolization using the self-expandable closed-cell stent for intracranial saccular aneurysm: a single-center experience of 289 consecutive aneurysms. Clin Radiol. 2013; 68:256–263.7. Mangubat EZ, Johnson AK, Keigher KM, Lopes DK. Initial Experience with Neuroform EZ in the Treatment of Wide-neck Cerebral Aneurysms. Neurointervention. 2012; 7:34–39.8. Starke RM, Durst CR, Evans A, Ding D, Raper DM, Jensen ME, et al. Endovascular treatment of unruptured wide-necked intracranial aneurysms: comparison of dual microcatheter technique and stent-assisted coil embolization. J Neurointerv Surg. 2015; 7:256–261.9. Pan J, Xiao F, Szeder V, Yan M, Fan W, Gu J, et al. Stent, balloon-assisted coiling and double microcatheter for treating wide-neck aneurysms in anterior cerebral circulation. Neurol Res. 2013; 35:1002–1008.10. Baxter BW, Rosso D, Lownie SP. Double microcatheter technique for detachable coil treatment of large, wide-necked intracranial aneurysms. AJNR Am J Neuroradiol. 1998; 19:1176–1178.11. Kwon OK, Kim SH, Kwon BJ, Kang HS, Kim JH, Oh CW, et al. Endovascular treatment of wide-necked aneurysms by using two microcatheters: techniques and outcomes in 25 patients. AJNR Am J Neuroradiol. 2005; 26:894–900.12. Lee JY, Seo JH, Cho YD, Kang HS, Han MH. Endovascular treatment of wide-neck intracranial aneurysms using a microcatheter protective technique: results and outcomes in 75 aneurysms. AJNR Am J Neuroradiol. 2011; 32:917–922.13. Kang HS, Kwon BJ, Kim JE, Han MH. Preinterventional clopidogrel response variability for coil embolization of intracranial aneurysms: clinical implications. AJNR Am J Neuroradiol. 2010; 31:1206–1210.14. Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003; 34:1398–1403.15. Kang HS, Han MH, Kwon BJ, Kwon OK, Kim SH, Choi SH, et al. Short-term outcome of intracranial aneurysms treated with polyglycolic acid/lactide copolymer-coated coils compared to historical controls treated with bare platinum coils: a single-center experience. AJNR Am J Neuroradiol. 2005; 26:1921–1928.16. Cho YD, Kang HS, Kim JE, Ahn JH, Jung SC, Kim CH, et al. Microguidewire protection of wide-necked aneurysms incorporating orifices of tortuous acute-angled vessels: a novel approach. Neuroradiology. 2014; 56:553–559.17. Cho YD, Lee WJ, Kim KM, Kang HS, Kim JE, Han MH. Endovascular coil embolization of middle cerebral artery aneurysms of the proximal (M1) segment. Neuroradiology. 2013; 55:1097–1102.18. Durst CR, Starke RM, Gaughen JR Jr, Geraghty S, Kreitel KD, Medel R, et al. Single-center experience with a dual microcatheter technique for the endovascular treatment of wide-necked aneurysms. J Neurosurg. 2014; 121:1093–1101.19. Kim DJ, Kim BM, Park KY, Ihm EH, Baek JH, Kim DI. Coil embolization of overwide and undertall small intracranial aneurysms with double microcatheter technique. Acta Neurochir (Wien). 2014; 156:839–846.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endovascular Treatment of Wide-Necked Intracranial Aneurysms : Techniques and Outcomes in 15 Patients
- A new definition for wide-necked cerebral aneurysms
- Endovascular Treatment of Cerebral Aneurysms: Coiling Techniques
- Usefulness of "Double-catheter" Technique in GDC Treatment of Intracranial Wide-necked Aneurysm
- Endovascular Treatment of Wide-Necked Intracranial Aneurysms Using Balloon-Assisted Technique with HyperForm Balloon
