Breast Microcalcifications: Diagnostic Outcomes According to Image-Guided Biopsy Method
- Affiliations
-
- 1Department of Radiology, Research Institute of Radiological Science, Yonsei University College of Medicine, Seoul 03722, Korea. ekkim@yuhs.ac
- KMID: 2160766
- DOI: http://doi.org/10.3348/kjr.2015.16.5.996
Abstract
OBJECTIVE
To evaluate the diagnostic outcomes of ultrasonography-guided core needle biopsy (US-CNB), US-guided vacuum-assisted biopsy (US-VAB), and stereotactic-guided vacuum-assisted biopsy (S-VAB) for diagnosing suspicious breast microcalcification.
MATERIALS AND METHODS
We retrospectively reviewed 336 cases of suspicious breast microcalcification in patients who subsequently underwent image-guided biopsy. US-CNB was performed for US-visible microcalcifications associated with a mass (n = 28), US-VAB for US-visible microcalcifications without an associated mass (n = 59), and S-VAB for mammogram-only visible lesions (n = 249). Mammographic findings, biopsy failure rate, false-negative rate, and underestimation rate were analyzed. Histological diagnoses and the Breast Imaging Reporting and Data System (BI-RADS) categories were reported.
RESULTS
Biopsy failure rates for US-CNB, US-VAB, and S-VAB were 7.1% (2/28), 0% (0/59), and 2.8% (7/249), respectively. Three false-negative cases were detected for US-CNB and two for S-VAB. The rates of biopsy-diagnosed ductal carcinoma in situ that were upgraded to invasive cancer at surgery were 41.7% (5/12), 12.9% (4/31), and 8.6% (3/35) for US-CNB, US-VAB, and S-VAB, respectively. Sonographically visible lesions were more likely to be malignant (66.2% [51/77] vs. 23.2% [46/198]; p < 0.001) or of higher BI-RADS category (61.0% [47/77] vs. 22.2% [44/198]; p < 0.001) than sonographically invisible lesions.
CONCLUSION
Ultrasonography-guided vacuum-assisted biopsy is more accurate than US-CNB when suspicious microcalcifications are detected on US. Calcifications with malignant pathology are significantly more visible on US than benign lesions.
MeSH Terms
Figure
-
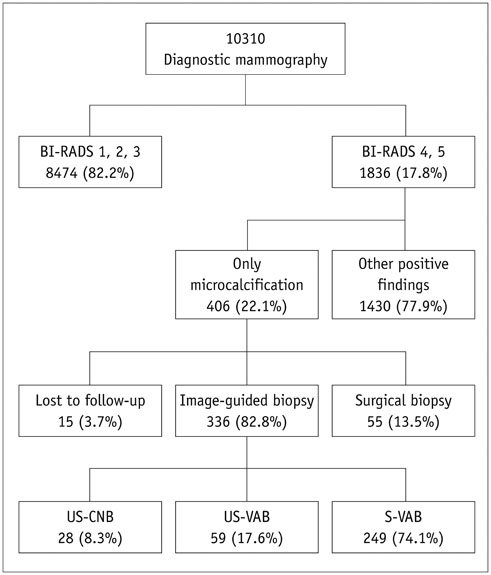
Fig. 1 Study population. BI-RADS = Breast Imaging Reporting and Data System, S-VAB = stereotactic-guided vacuum assisted biopsy, US-CNB = ultrasonography-guided core needle biopsy, US-VAB = ultrasonography-guided vacuum assisted biopsy
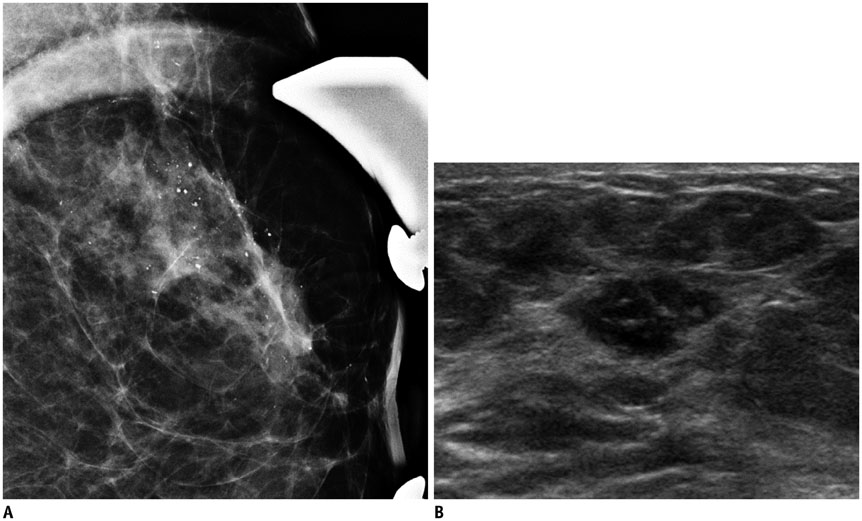
Fig. 2 68-year-old female patient with complaint of bloody nipple discharge from left breast. A. Magnified mammogram of left breast reveals suspicious segmental coarse heterogeneous microcalcifications. B. Ultrasonogram of left breast shows hypoechoic mass with internal hyperechoic foci in upper outer aspect of left breast. 14-gauge ultrasonography-guided core needle biopsy was performed on mass, and final diagnosis was invasive ductal carcinoma.
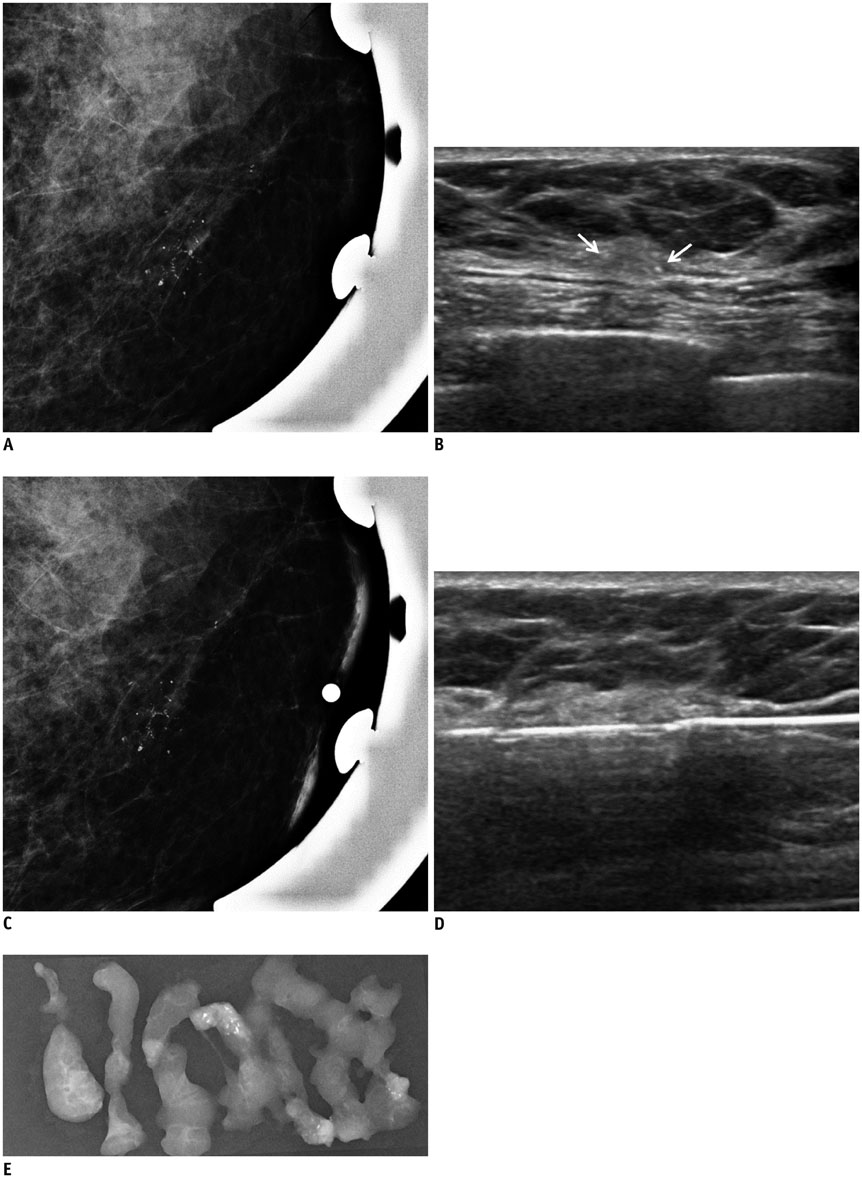
Fig. 3 54-year-old female patient who underwent screening mammography. A. Magnified mammogram of left breast reveals suspicious segmental coarse heterogeneous microcalcifications. B. Ultrasonogram of left breast shows microcalcifications (arrows) at corresponding area of microcalcifications observed on mammography. C. Radio-opaque marker was placed on skin over lesion for confirmation, and left breast view was magnified. Ultrasonography (US)-visible microcalcifications are correlated with mammographically visualized microcalcifications. D. 11-gauge US-guided vacuum-assisted biopsy is performed. E. Specimen mammography confirms retrieval of microcalcifications. Diagnosis was ductal carcinoma in situ, which was also confirmed by post-partial mastectomy pathology.
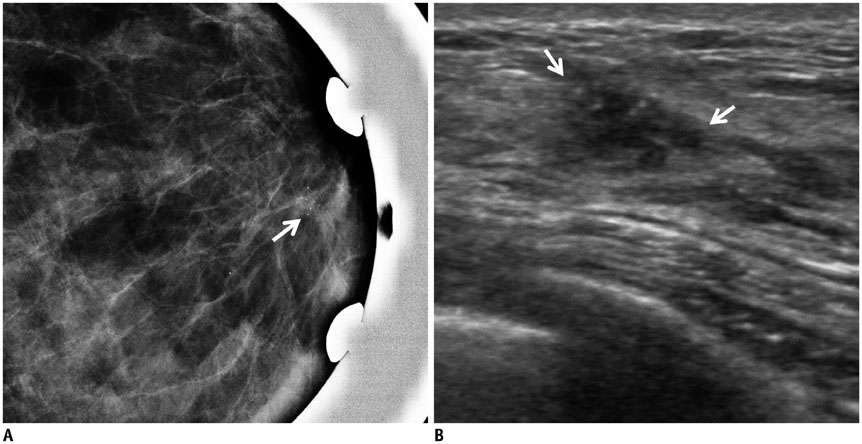
Fig. 4 47-year-old female patient who underwent screening mammography. A. Magnified mammogram of left breast reveals suspicious grouped fine pleomorphic microcalcifications (arrow). B. Ultrasonogram of left breast shows hypoechoic mass with internal hyperechoic foci (arrows) in upper central aspect of left breast. 14-gauge ultrasonography-guided core needle biopsy was performed on mass, and calcifications were not retrieved per specimen mammography. Diagnosis was stromal fibrosis, which was thought to be discordant with imaging findings. Patient underwent excisional biopsy under wire localization, and final diagnosis was ductal carcinoma in situ.
Cited by 2 articles
-
Annual Trends in Ultrasonography-Guided 14-Gauge Core Needle Biopsy for Breast Lesions
Inha Jung, Kyunghwa Han, Min Jung Kim, Hee Jung Moon, Jung Hyun Yoon, Vivian Youngjean Park, Eun-Kyung Kim
Korean J Radiol. 2020;21(3):259-267. doi: 10.3348/kjr.2019.0695.The Utility of MicroPure™ Ultrasound Technique in Assessing Grouped Microcalcifications without a Mass on Mammography
Ah Young Park, Bo Kyoung Seo, Kyu Ran Cho, Ok Hee Woo
J Breast Cancer. 2016;19(1):83-86. doi: 10.4048/jbc.2016.19.1.83.
Reference
-
1. Anania G, Bazzocchi M, di Loreto C, Risaliti A, Terrosu G, Donini A, et al. Percutaneous large core needle biopsy versus surgical biopsy in the diagnosis of breast lesions. Int Surg. 1997; 82:52–55.2. Elvecrog EL, Lechner MC, Nelson MT. Nonpalpable breast lesions: correlation of stereotaxic large-core needle biopsy and surgical biopsy results. Radiology. 1993; 188:453–455.3. Gisvold JJ, Goellner JR, Grant CS, Donohue JH, Sykes MW, Karsell PR, et al. Breast biopsy: a comparative study of stereotaxically guided core and excisional techniques. AJR Am J Roentgenol. 1994; 162:815–820.4. Park JS, Park YM, Kim EK, Kim SJ, Han SS, Lee SJ, et al. Sonographic findings of high-grade and non-high-grade ductal carcinoma in situ of the breast. J Ultrasound Med. 2010; 29:1687–1697.5. Soo MS, Baker JA, Rosen EL. Sonographic detection and sonographically guided biopsy of breast microcalcifications. AJR Am J Roentgenol. 2003; 180:941–948.6. Yu PC, Lee YW, Chou FF, Wu SC, Huang CC, Ng SH, et al. Clustered microcalcifications of intermediate concern detected on digital mammography: ultrasound assessment. Breast. 2011; 20:495–500.7. Parker SH, Burbank F. A practical approach to minimally invasive breast biopsy. Radiology. 1996; 200:11–20.8. Soo MS, Baker JA, Rosen EL, Vo TT. Sonographically guided biopsy of suspicious microcalcifications of the breast: a pilot study. AJR Am J Roentgenol. 2002; 178:1007–1015.9. Cho N, Moon WK, Cha JH, Kim SM, Jang M, Chang JM, et al. Ultrasound-guided vacuum-assisted biopsy of microcalcifications detected at screening mammography. Acta Radiol. 2009; 50:602–609.10. Kim HS, Kim MJ, Kim EK, Kwak JY, Son EJ, Oh KK. US-guided vacuum-assisted biopsy of microcalcifications in breast lesions and long-term follow-up results. Korean J Radiol. 2008; 9:503–509.11. Yi J, Lee EH, Kwak JJ, Cha JG, Jung SH. Retrieval rate and accuracy of ultrasound-guided 14-G semi-automated core needle biopsy of breast microcalcifications. Korean J Radiol. 2014; 15:12–19.12. Kettritz U, Rotter K, Schreer I, Murauer M, Schulz-Wendtland R, Peter D, et al. Stereotactic vacuum-assisted breast biopsy in 2874 patients: a multicenter study. Cancer. 2004; 100:245–251.13. Zuiani C, Mazzarella F, Londero V, Linda A, Puglisi F, Bazzocchi M. Stereotactic vacuum-assisted breast biopsy: results, follow-up and correlation with radiological suspicion. Radiol Med. 2007; 112:304–317.14. Golub RM, Bennett CL, Stinson T, Venta L, Morrow M. Cost minimization study of image-guided core biopsy versus surgical excisional biopsy for women with abnormal mammograms. J Clin Oncol. 2004; 22:2430–2437.15. Hahn SY, Shin JH, Han BK, Ko EY. Sonographically-guided vacuum-assisted biopsy with digital mammography-guided skin marking of suspicious breast microcalcifications: comparison of outcomes with stereotactic biopsy in Asian women. Acta Radiol. 2011; 52:29–34.16. Jung YJ, Bae YT, Lee JY, Seo HI, Kim JY, Choo KS. Lateral decubitus positioning stereotactic vacuum-assisted breast biopsy with true lateral mammography. J Breast Cancer. 2011; 14:64–68.17. Burbank F, Parker SH. Methods for Analysis of One-Step Breast Biopsy Programs. Breast J. 1998; 4:307–319.18. Wunderbaldinger P, Wolf G, Turetschek K, Helbich TH. Comparison of sitting versus prone position for stereotactic large-core breast biopsy in surgically proven lesions. AJR Am J Roentgenol. 2002; 178:1221–1225.19. Jackman RJ, Rodriguez-Soto J. Breast microcalcifications: retrieval failure at prone stereotactic core and vacuum breast biopsy--frequency, causes, and outcome. Radiology. 2006; 239:61–70.20. Schrading S, Distelmaier M, Dirrichs T, Detering S, Brolund L, Strobel K, et al. Digital breast tomosynthesis-guided vacuum-assisted breast biopsy: initial experiences and comparison with prone stereotactic vacuum-assisted biopsy. Radiology. 2015; 274:654–662.21. Welle GJ, Clark M, Loos S, Pauls D, Warden D, Sheffield M, et al. Stereotactic breast biopsy: recumbent biopsy using add-on upright equipment. AJR Am J Roentgenol. 2000; 175:59–63.22. Jackman RJ, Nowels KW, Rodriguez-Soto J, Marzoni FA Jr, Finkelstein SI, Shepard MJ. Stereotactic, automated, large-core needle biopsy of nonpalpable breast lesions: false-negative and histologic underestimation rates after long-term follow-up. Radiology. 1999; 210:799–805.23. Lee CH, Philpotts LE, Horvath LJ, Tocino I. Follow-up of breast lesions diagnosed as benign with stereotactic core-needle biopsy: frequency of mammographic change and false-negative rate. Radiology. 1999; 212:189–194.24. Crystal P, Koretz M, Shcharynsky S, Makarov V, Strano S. Accuracy of sonographically guided 14-gauge core-needle biopsy: results of 715 consecutive breast biopsies with at least two-year follow-up of benign lesions. J Clin Ultrasound. 2005; 33:47–52.25. Cho N, Moon WK. Digital mammography-guided skin marking for sonographically guided biopsy of suspicious microcalcifications. AJR Am J Roentgenol. 2009; 192:W132–W136.26. Jackman RJ, Burbank F, Parker SH, Evans WP 3rd, Lechner MC, Richardson TR, et al. Stereotactic breast biopsy of nonpalpable lesions: determinants of ductal carcinoma in situ underestimation rates. Radiology. 2001; 218:497–502.27. Moon WK, Im JG, Koh YH, Noh DY, Park IA. US of mammographically detected clustered microcalcifications. Radiology. 2000; 217:849–854.28. Wang LC, Sullivan M, Du H, Feldman MI, Mendelson EB. US appearance of ductal carcinoma in situ. Radiographics. 2013; 33:213–228.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Results of Mammography and Ultrasound-Guided Localization Biopsy of Nonpalpable Breast Lesions, and the Differences between Them
- Calcifications on Breast Ultrasonography
- Ultrasonographically-Guided Biopsy after Digital Mammographically Guided Two-Dimensional Localization of Breast Microcalcifications
- Clinical Implication of Intraoperative Sonography in Localized Excision Biopsy for Mammographic Microcalcifications
- Interpretation of ImageGuided Biopsy Results and Assessment
